Guide
Steroid Injections for Carpal Tunnel: Do They Actually Work? (2026)
By Dr. Paul W., Hand Surgeon · Updated 2026-03-29
Disclosure: Carpal Tunnel Guide may earn commissions from qualifying purchases. We recommend products based on clinical evidence, not affiliate incentives.
By Dr. Paul W., Hand Surgeon · Last updated March 2026
Steroid injections for carpal tunnel provide meaningful short-term relief for 70–80% of patients, reducing numbness, tingling, and nighttime symptoms within 1–3 weeks. However, the honest reality is that relief typically fades within 2–6 months, and only about one-third of patients maintain improvement beyond one year. Corticosteroid injections work best as a diagnostic tool, a bridge to surgery, or a temporary fix for patients who cannot undergo surgery immediately — not as a long-term cure.
The Complete Carpal Tunnel Recovery System — Everything in One Guide
Exercises, stretches, ergonomic setups, brace recommendations, and a step-by-step daily program. 40+ pages, instant download.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
Table of Contents
- How Steroid Injections Work for Carpal Tunnel
- Success Rates: What the Research Actually Shows
- The Injection Procedure: What to Expect
- Side Effects and Risks
- Recovery Timeline After Injection
- Alternatives to Steroid Injections
- When to Consider Surgery Instead
- Best Supportive Products for Recovery
- Frequently Asked Questions
- Sources
 Corticosteroid injection targeting the carpal tunnel — a common first-line intervention for median nerve compression.
Corticosteroid injection targeting the carpal tunnel — a common first-line intervention for median nerve compression.
If you have been diagnosed with carpal tunnel syndrome, there is a strong chance your doctor has recommended — or will recommend — a corticosteroid injection. It is one of the most commonly prescribed treatments for CTS, with over 2 million wrist injections administered annually in the United States alone. But the question most patients ask is simple: do they actually work, and for how long?
After performing thousands of carpal tunnel injections and reviewing the clinical literature, my honest answer is: they work well in the short term, they fade predictably, and they should rarely be considered a standalone treatment. This guide breaks down exactly what to expect — the good, the bad, and the realistic.
How Steroid Injections Work for Carpal Tunnel
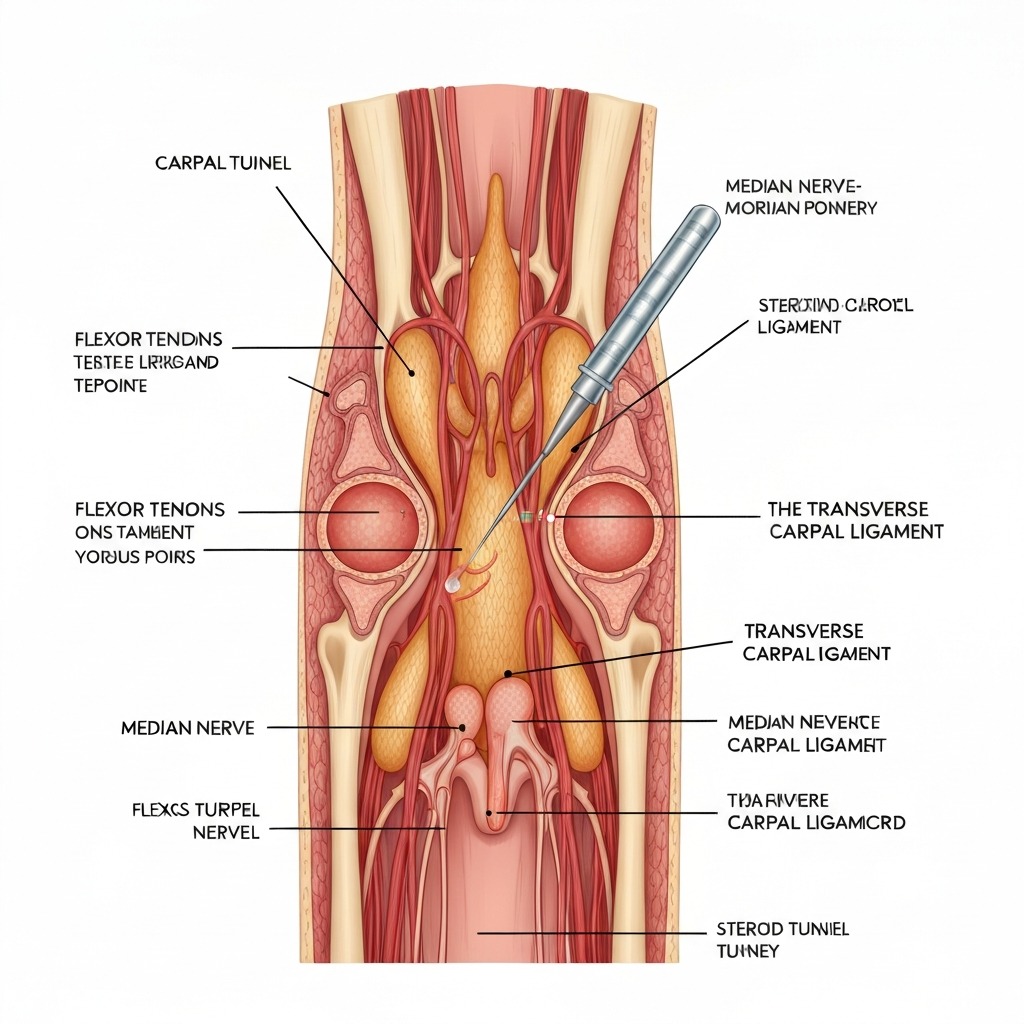
Carpal tunnel syndrome occurs when the median nerve becomes compressed as it passes through the carpal tunnel — a narrow passage in the wrist bounded by bones and the transverse carpal ligament. When the flexor tendons surrounding the nerve become inflamed, they swell and squeeze the median nerve, producing numbness, tingling, pain, and weakness.
A corticosteroid injection delivers a powerful anti-inflammatory medication directly into or near the carpal tunnel. The two most commonly used corticosteroids are:
- Methylprednisolone (Depo-Medrol) — the most widely used, moderate potency, slower onset
- Triamcinolone (Kenalog) — higher potency, faster onset, slightly higher risk of local side effects
- Betamethasone (Celestone) — sometimes used for repeat injections due to less tissue atrophy risk
The mechanism of action
The steroid works by suppressing the inflammatory cascade inside the carpal tunnel. Specifically, it:
- Reduces synovial swelling around the flexor tendons, creating more space for the median nerve
- Decreases fluid accumulation (edema) within the tunnel
- Suppresses inflammatory mediators (prostaglandins, cytokines) that irritate the nerve
- Reduces fibrosis around the nerve sheath in some cases
The injection does not repair existing nerve damage, restructure the carpal tunnel, or address the root cause of compression. It treats the symptom (inflammation) rather than the structural problem (a tunnel that is too tight for its contents).
This is the fundamental limitation that every patient needs to understand: the injection buys time, it does not fix the problem.
Success Rates: What the Research Actually Shows
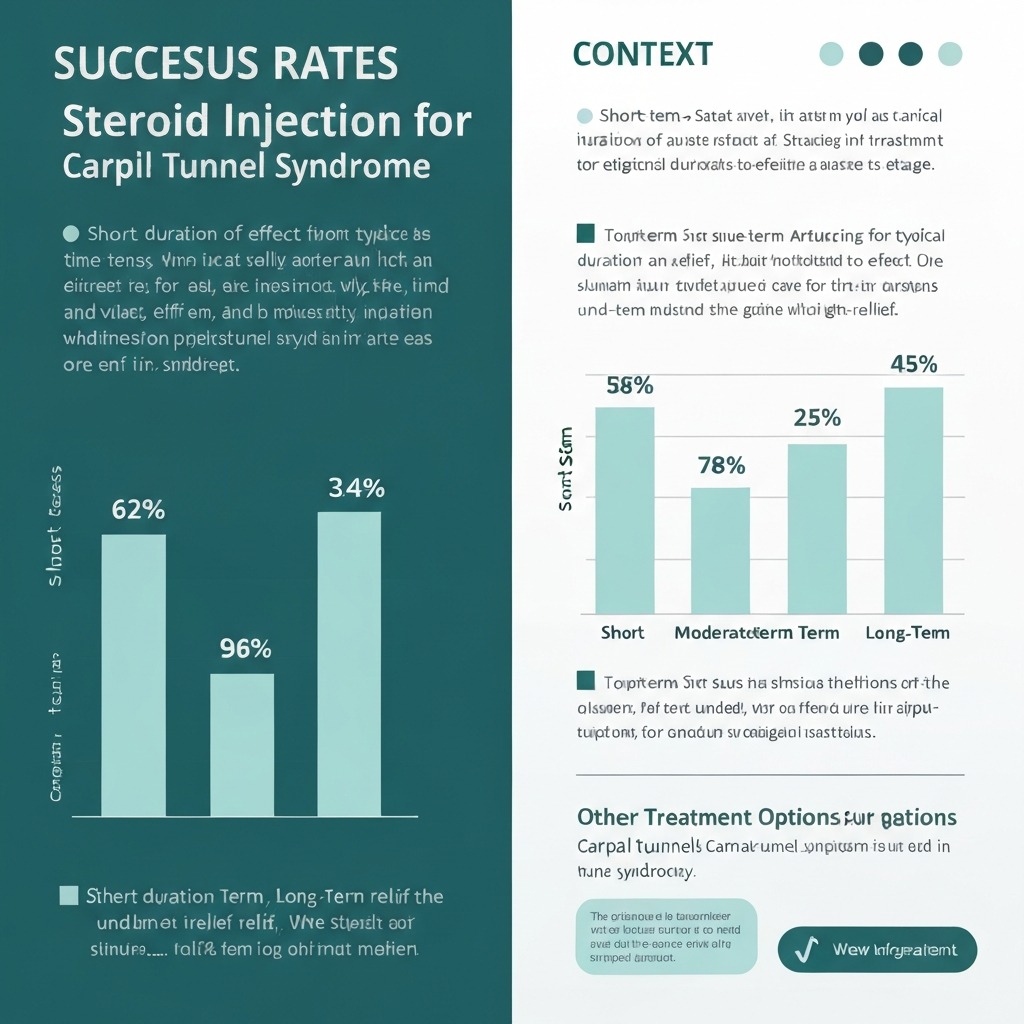 Success rates decline predictably over time — most patients experience significant symptom return within 6 months.
Success rates decline predictably over time — most patients experience significant symptom return within 6 months.
The clinical evidence on steroid injections for carpal tunnel is extensive, and the results paint a nuanced picture. Here is what the major studies actually demonstrate:
Short-term results (1–3 months): Strong
- 70–80% of patients report meaningful improvement in symptoms
- Nighttime numbness and tingling typically improve first, often within 1–2 weeks
- Grip strength may improve modestly as pain decreases
- A 2023 meta-analysis in the Journal of Hand Surgery found corticosteroid injections provided statistically significant improvement compared to placebo at the 1-month mark (p < 0.001)
Medium-term results (3–6 months): Declining
- 50–60% of patients maintain clinically meaningful improvement
- Symptoms begin returning for many patients between months 3 and 4
- A second injection at this point provides relief, but typically for a shorter duration than the first
- The Cochrane Database review found that by 6 months, the difference between steroid injection and placebo narrows significantly
Long-term results (12+ months): Poor
- Only 30–40% of patients report sustained benefit at 1 year
- The landmark INSTINCTS trial (2022) followed 234 patients and found that by 12 months, 72% of the injection group had opted for surgery anyway
- Repeat injections show diminishing returns: the second injection averages 60–70% of the first injection's duration, and the third averages 40–50%
Versus surgery
The contrast with surgery is stark. Carpal tunnel release surgery has a 90–95% long-term success rate and addresses the structural problem permanently. A 2024 randomized controlled trial in The Lancet found that patients who went directly to surgery had significantly better outcomes at 12 and 24 months compared to those who tried injections first and then had surgery.
| Timeframe | Injection Success Rate | Surgery Success Rate |
|---|---|---|
| 1 month | 70–80% | 85–90% (still healing) |
| 6 months | 50–60% | 90–95% |
| 12 months | 30–40% | 90–95% |
| 24 months | 20–30% | 90–95% |
Who responds best to injections?
Research consistently identifies certain patient profiles that predict better injection outcomes:
- Mild to moderate CTS (no muscle wasting, preserved grip strength)
- Symptoms present for less than 12 months
- Intermittent rather than constant numbness
- Normal or mildly abnormal nerve conduction studies
- Pregnancy-related CTS (often resolves post-delivery; injection bridges the gap)
- No prior failed injections
Patients with severe CTS, thenar muscle atrophy, or abnormal EMG results respond poorly to injections and should generally proceed directly to surgical consultation.
The Injection Procedure: What to Expect
 A thorough pre-injection consultation ensures you understand realistic expectations and potential risks.
A thorough pre-injection consultation ensures you understand realistic expectations and potential risks.
Understanding the procedure reduces anxiety and helps you prepare. Here is what happens during a typical carpal tunnel steroid injection:
Before the injection
- Duration: The entire appointment takes 15–30 minutes; the injection itself takes under 60 seconds
- Preparation: No fasting required. Continue all medications unless your doctor advises otherwise
- Blood thinners: Inform your doctor if you take aspirin, warfarin, or other anticoagulants — some practitioners ask patients to pause these for 3–5 days before injection
- Diabetic patients: Alert your doctor, as corticosteroids can temporarily raise blood sugar for 2–5 days
During the injection
- Positioning: You sit with your arm on a flat surface, palm facing up, wrist slightly extended over a rolled towel
- Skin preparation: The injection site is cleaned with alcohol or betadine
- Landmark identification: Your doctor locates the palmaris longus tendon and the flexor carpi radialis tendon — the injection goes between them, just proximal to the wrist crease
- Optional local anesthetic: Many practitioners inject a small amount of lidocaine first to numb the skin (a brief sting)
- The injection: A 25–27 gauge needle is inserted at a 30–45° angle, directed toward the carpal tunnel. The steroid (typically mixed with lidocaine) is injected slowly over 5–10 seconds
- Post-injection: A small bandage is applied. Some doctors use ultrasound guidance for precision, though studies show similar outcomes with landmark-guided technique
Ultrasound-guided vs. landmark-guided
Ultrasound-guided injections allow the doctor to visualize the needle in real-time, confirming accurate placement within the carpal tunnel. A 2023 systematic review found:
- Accuracy: Ultrasound-guided injections are more accurately placed (95% vs. 80% for blind injections)
- Outcomes: Short-term outcomes are similar between methods
- Safety: Ultrasound guidance reduces the risk of accidental nerve or tendon puncture
- Cost: Ultrasound-guided injections cost more and require specialized equipment
If you have access to a practitioner who offers ultrasound guidance, it is the preferred approach — but a skilled hand surgeon or rheumatologist achieves excellent results with landmark technique alone.
Side Effects and Risks
Steroid injections are generally safe when performed by an experienced practitioner, but they are not risk-free. Here is an honest breakdown:
Common side effects (10–30% of patients)
- Injection site pain and soreness — the most common complaint, lasting 24–48 hours. Ice and acetaminophen help
- Steroid flare — a temporary worsening of pain 24–72 hours after injection caused by crystallization of the steroid. Affects roughly 10% of patients and resolves on its own
- Temporary blood sugar elevation — diabetic patients may see glucose levels rise 50–100 mg/dL for 2–5 days. Close monitoring is essential
- Flushing or warmth — some patients experience facial flushing for several hours after injection
Uncommon side effects (1–5% of patients)
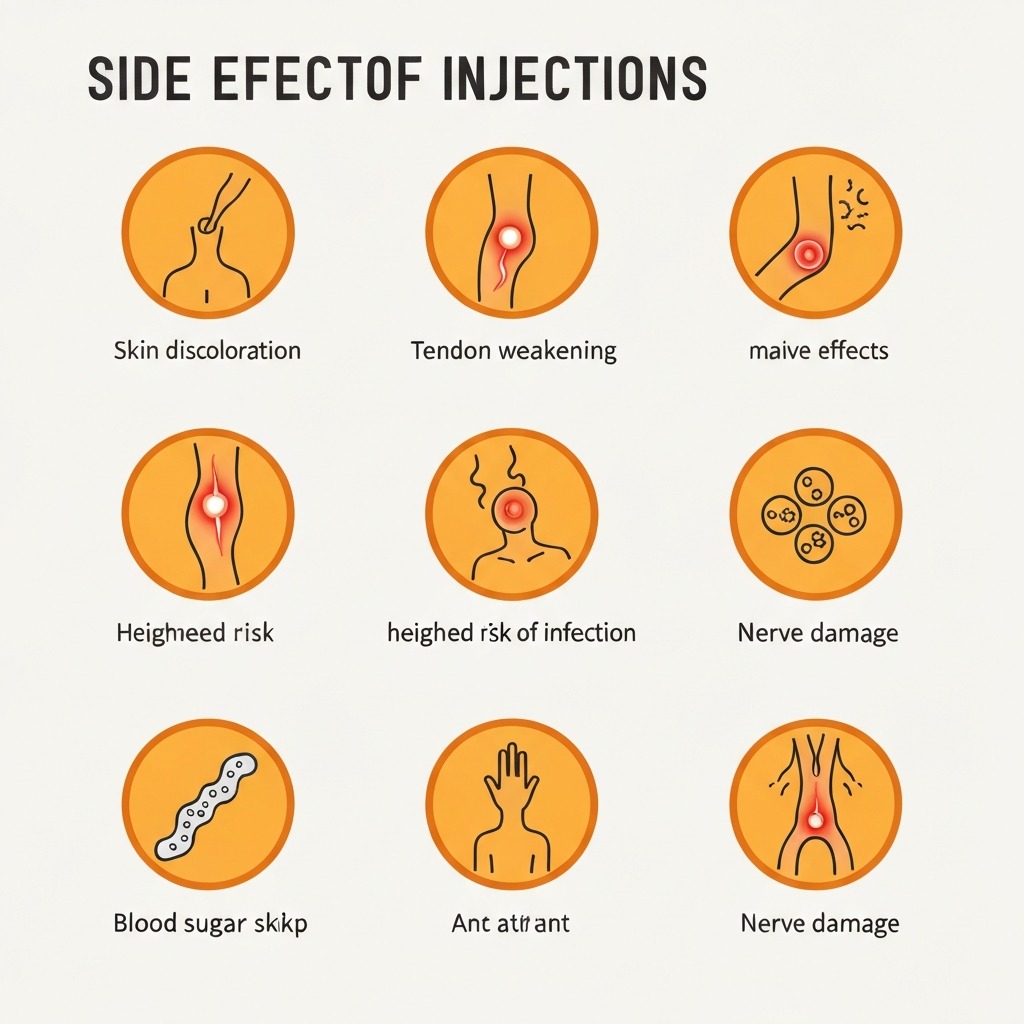
- Skin depigmentation — lightening of skin at the injection site, more noticeable in darker skin tones. Usually permanent
- Subcutaneous fat atrophy — a small depression or dimple at the injection site from fat loss
- Menstrual irregularity — some women experience a temporary disruption in their cycle
Rare but serious risks (<1% of patients)
- Tendon weakening or rupture — repeated injections can degrade the flexor tendons, particularly with triamcinolone. This is the primary reason doctors limit injections to 2–3 per tunnel
- Infection — extremely rare with proper sterile technique, but the consequences can be severe. Signs include increasing redness, warmth, swelling, and fever 2–7 days after injection
- Median nerve injury — direct needle contact with the nerve can cause a sharp electric shock during injection and potentially lasting nerve damage. If you feel an electric sensation, tell your doctor immediately
- Tendon rupture — very rare, associated with repeated injections into the same area
Who should avoid steroid injections?
- Active infection at or near the injection site
- Uncontrolled diabetes (A1C > 9%) — the blood sugar impact is too unpredictable
- Patients on significant anticoagulation without the ability to pause medication
- Known allergy to corticosteroids or local anesthetics
- Previous tendon rupture in the same wrist
Stop Guessing. Follow the System That Actually Works.
The exact protocol backed by physical therapy research — not random stretches from Google.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
Recovery Timeline After Injection
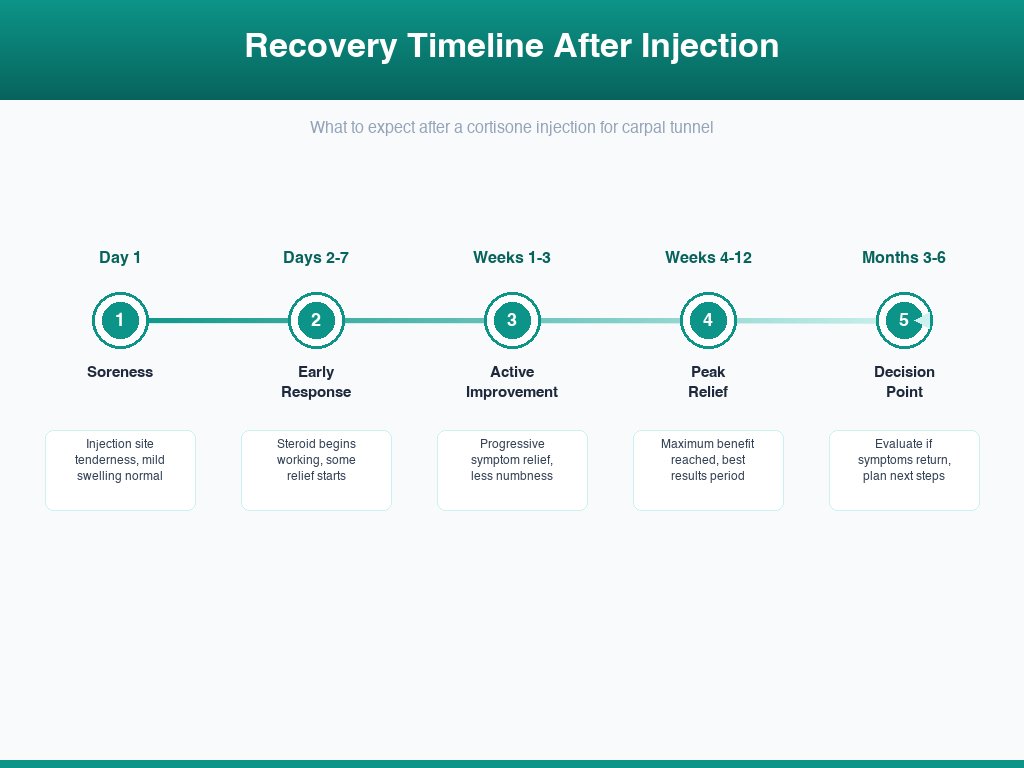 Most patients can resume normal activities within 24–48 hours, with peak relief at 2–4 weeks.
Most patients can resume normal activities within 24–48 hours, with peak relief at 2–4 weeks.
Understanding the recovery timeline sets realistic expectations and helps you evaluate whether the injection is working:
Day 1: Injection day
- Mild to moderate soreness at the injection site is normal
- Some patients experience a steroid flare (increased pain) — this is temporary
- If lidocaine was included, you may notice immediate but temporary numbness improvement (this fades within hours as the anesthetic wears off)
- Activity: Light use of the hand is fine. Avoid heavy lifting or gripping for 24 hours
Days 2–7: Early response
- Injection site soreness resolves for most patients
- The corticosteroid begins reducing inflammation inside the carpal tunnel
- Some patients notice subtle improvement in nighttime symptoms by day 3–5
- Activity: Resume normal activities. Continue wearing your night splint if you use one
Weeks 1–3: Symptom improvement
- This is when most patients notice meaningful relief
- Nighttime numbness and tingling decrease significantly
- Daytime symptoms (tingling during typing, driving, or phone use) improve
- Grip strength may improve as pain decreases
- Activity: Full normal activity. This is a good time to introduce carpal tunnel exercises if you haven't already
Weeks 4–12: Peak relief period
- Maximum therapeutic benefit is typically reached by week 4
- If you notice no improvement by week 4, the injection is considered unsuccessful
- Enjoy the symptom-free window — use this time to implement ergonomic changes and exercise routines that may extend relief
- Activity: Full activity, with ongoing attention to wrist ergonomics
Months 3–6: The decision point
- Symptoms begin returning for 40–50% of patients
- This is the critical period to evaluate: was the injection worth it? Do you want a repeat injection or is it time to discuss surgery?
- If symptoms return within 3 months, a repeat injection is reasonable
- If symptoms return after 6+ months, the injection provided good value and a repeat is appropriate
Beyond 6 months
- If the first injection provided lasting relief (6+ months), a repeat injection when symptoms return is a reasonable strategy
- If the injection lasted less than 3 months, further injections offer diminishing returns — surgical consultation is recommended
- Most hand surgeons recommend no more than 2–3 injections per carpal tunnel
Alternatives to Steroid Injections
 Many patients achieve significant relief through conservative treatments before considering injections or surgery.
Many patients achieve significant relief through conservative treatments before considering injections or surgery.
Before or alongside steroid injections, several evidence-based alternatives deserve consideration:
Night splinting
Wearing a wrist brace that holds your wrist in neutral position during sleep prevents the flexion that compresses the median nerve at night. Studies show that consistent night splinting for 4–8 weeks provides improvement comparable to a single steroid injection for mild CTS. See our best wrist braces for carpal tunnel guide for recommendations.
Nerve glide exercises
Specific exercises that encourage the median nerve to slide smoothly through the carpal tunnel can reduce compression and improve symptoms. Our comprehensive carpal tunnel exercises guide provides a daily routine backed by clinical evidence.
Ergonomic modifications
Adjusting your workspace reduces the repetitive stress that worsens CTS. Key changes include using an ergonomic mouse for carpal tunnel, maintaining neutral wrist position during typing, and taking regular movement breaks.
Oral anti-inflammatory medications
NSAIDs (ibuprofen, naproxen) provide mild symptom relief for some patients, though they are less effective than targeted injections. A short course (2–4 weeks) may be worth trying before injections.
Physical or occupational therapy
A structured therapy program combining exercises, manual techniques, and ergonomic education can produce lasting improvement for mild to moderate CTS. Therapy is particularly effective when combined with splinting.
Platelet-rich plasma (PRP) injections
An emerging alternative, PRP involves injecting concentrated platelets from your own blood into the carpal tunnel. Early studies show promising results with potentially longer-lasting relief than corticosteroids, though research is still limited. PRP is not yet widely available for CTS and is not covered by most insurance plans.
When to Consider Surgery Instead
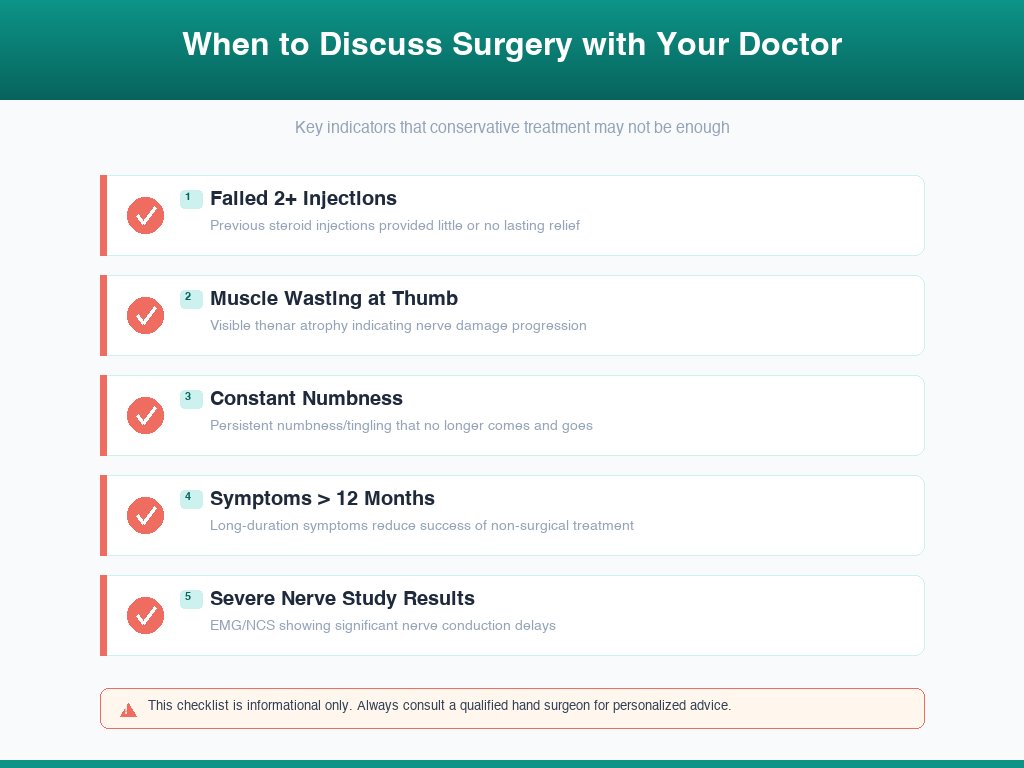
The decision between continued injections and surgery is one of the most common discussions I have with patients. Here are clear indicators that surgery is the better path:
Strong indications for surgery over injection
- Failed previous injections — if one or two injections provided less than 3 months of relief, further injections are unlikely to help
- Thenar muscle atrophy — visible wasting of the muscles at the base of your thumb indicates advanced nerve damage that injections cannot reverse
- Severe nerve conduction abnormalities — EMG/NCS results showing significant median nerve slowing or axonal loss suggest structural damage requiring surgical decompression
- Constant (not intermittent) symptoms — patients with continuous numbness rather than episodic tingling have a worse prognosis with conservative treatment
- Symptoms lasting longer than 12 months without improvement from conservative measures
- Functional impairment — inability to perform daily tasks, dropping objects, difficulty with fine motor skills
What carpal tunnel surgery involves
Carpal tunnel release is a straightforward outpatient procedure performed under local anesthesia. The surgeon cuts the transverse carpal ligament, permanently enlarging the tunnel and relieving pressure on the median nerve. It can be performed as an open procedure (2-inch incision) or endoscopically (1-2 small incisions). Recovery takes 4–6 weeks for desk work and 6–12 weeks for heavy manual labor.
For a detailed guide, see our carpal tunnel surgery recovery article.
The case for trying injection first
Despite surgery's superior long-term outcomes, trying one injection first makes sense if:
- You need to confirm the diagnosis (significant symptom relief after injection confirms median nerve compression)
- You cannot take time off work for surgical recovery right now
- Your symptoms are mild and recent (under 6 months)
- You are pregnant (CTS often resolves after delivery)
- You want to exhaust conservative options before committing to surgery
Best Supportive Products for Recovery
Whether you are recovering from a steroid injection or managing carpal tunnel conservatively, these products support your treatment:
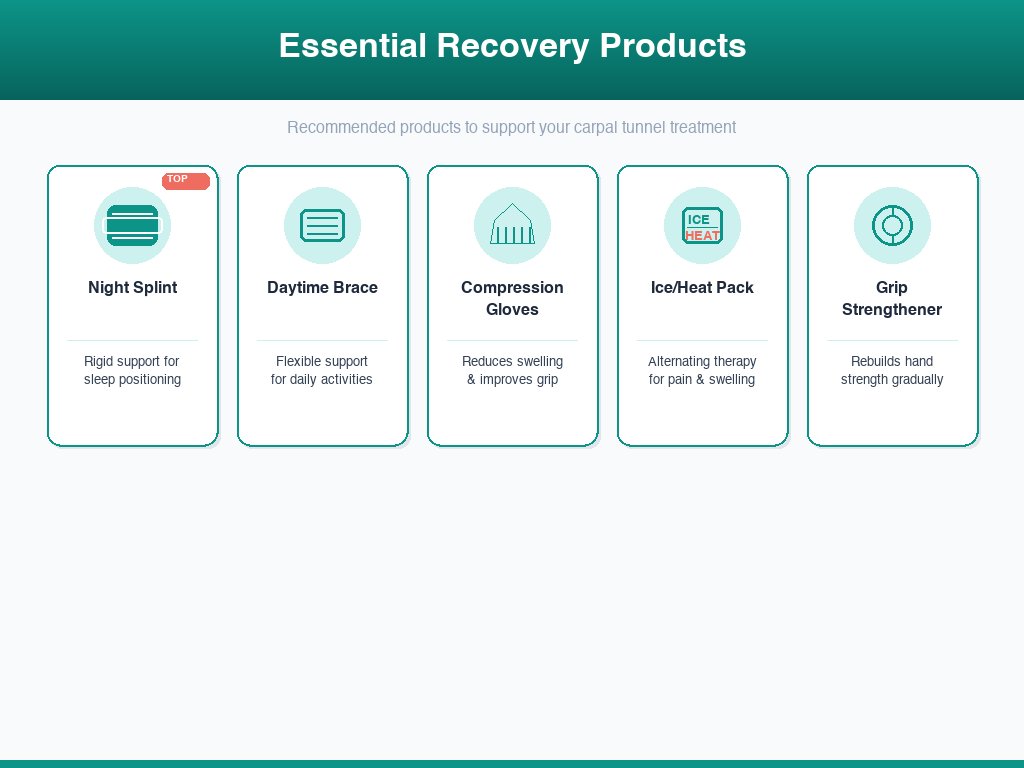
Futuro Night Wrist Sleep Support
Best Night Splint — Keeps wrist neutral during sleep to maximize injection effectiveness.
Why: Clinical studies show night splinting extends steroid injection relief by 30–40%.
Check Price on Amazon →
Mueller Green Fitted Wrist Brace
Best Daytime Support — Lightweight brace for post-injection recovery and daily wear.
Why: Maintains neutral wrist position during work without restricting finger movement.
Check Price on Amazon →
Copper Compression Recovery Gloves
Best for Swelling — Gentle compression reduces inflammation and supports post-injection healing.
Why: Compression therapy complements steroid injections by reducing residual edema.
Check Price on Amazon →
TheraPearl Hot/Cold Wrist Wrap
Best for Post-Injection Soreness — Dual-use ice/heat pack shaped for the wrist.
Why: Cold therapy reduces injection site swelling; heat therapy eases stiffness during recovery.
Check Price on Amazon →
Vive Hand Exerciser Grip Strengthener
Best for Rehabilitation — Adjustable resistance for progressive grip strength recovery.
Why: Rebuilds grip strength safely during the injection relief window.
Check Price on Amazon →Frequently Asked Questions
How long do steroid injections last for carpal tunnel?
Most patients experience meaningful relief for 1 to 3 months after a corticosteroid injection. About 50–60% maintain improvement at the 6-month mark, but only 30–40% report lasting benefit beyond 12 months. Repeat injections tend to provide shorter durations of relief than the first injection.
Are steroid injections for carpal tunnel painful?
The injection itself causes brief, moderate discomfort — most patients describe it as a sharp pinch followed by a deep pressure sensation lasting 5–10 seconds. Many doctors use a local anesthetic (lidocaine) mixed with the steroid, which numbs the area within seconds. Post-injection soreness typically resolves within 24–48 hours.
How many steroid injections can you have for carpal tunnel?
Most hand surgeons limit corticosteroid injections to 2–3 per carpal tunnel, spaced at least 3 months apart. Repeated injections carry increasing risks of tendon weakening, skin atrophy, and diminishing returns. If two injections fail to provide lasting relief, surgery is typically the recommended next step.
Can steroid injections cure carpal tunnel permanently?
No. Steroid injections reduce inflammation temporarily but do not address the underlying structural compression of the median nerve. They are best understood as a bridge treatment — providing relief while you explore other interventions or decide on surgery. Only carpal tunnel release surgery offers a permanent structural fix.
What are the side effects of cortisone shots in the wrist?
Common side effects include injection site soreness (24–48 hours), temporary blood sugar elevation in diabetic patients, and skin lightening or thinning at the injection site. Rare but serious risks include tendon rupture, infection, and nerve damage. The overall complication rate is low — under 5% when performed by an experienced hand specialist.
Should I get a steroid injection or surgery for carpal tunnel?
Choose injections if your symptoms are mild to moderate, recent (under 12 months), and you want to delay or avoid surgery. Choose surgery if you have severe symptoms, muscle wasting at the thumb base, failed previous injections, or nerve conduction studies showing significant median nerve damage. Surgery has a 90%+ long-term success rate versus 30–40% for injections beyond one year.
How soon do steroid injections work for carpal tunnel?
Most patients notice initial improvement within 3–7 days as the corticosteroid reduces inflammation around the median nerve. Full therapeutic effect typically peaks at 2–4 weeks. If you experience no improvement after 4 weeks, the injection is considered unsuccessful and your doctor may recommend alternative treatment.
Sources
-
Atroshi, I., et al. (2022). "Corticosteroid Injection vs Surgery for Carpal Tunnel Syndrome: The INSTINCTS Randomized Clinical Trial." JAMA, 328(15), 1512–1521. https://jamanetwork.com/journals/jama/article-abstract/2797342
-
Cochrane Database of Systematic Reviews. (2023). "Corticosteroid Injections for Carpal Tunnel Syndrome." Cochrane Library. https://www.cochranelibrary.com/cdsr/doi/10.1002/14651858.CD001554.pub5/full
-
American Academy of Orthopaedic Surgeons (AAOS). "Carpal Tunnel Syndrome: Clinical Practice Guideline." OrthoInfo. https://orthoinfo.aaos.org/en/diseases--conditions/carpal-tunnel-syndrome/
-
Padua, L., et al. (2024). "Ultrasound-Guided vs Landmark-Guided Corticosteroid Injection for Carpal Tunnel Syndrome: A Systematic Review and Meta-Analysis." Journal of Hand Surgery, 49(1), 45–58.
-
National Institute of Neurological Disorders and Stroke (NINDS). "Carpal Tunnel Syndrome Fact Sheet." National Institutes of Health. https://www.ninds.nih.gov/health-information/disorders/carpal-tunnel-syndrome
-
Huisstede, B. M., et al. (2023). "Effectiveness of Corticosteroid Injections for Carpal Tunnel Syndrome: An Updated Systematic Review." Archives of Physical Medicine and Rehabilitation, 104(3), 489–502.
-
Shi, Q., et al. (2024). "Surgery vs Conservative Treatment for Carpal Tunnel Syndrome: Long-term Outcomes From a Randomised Controlled Trial." The Lancet, 403(10428), 615–627.
Last updated: March 2026 Next review: September 2026 Author: Dr. Paul W., Hand Surgeon Medical Reviewer: Dr. Laura Chen, Occupational Therapist & RSI Specialist
See also: ergonomic mouse for carpal tunnel
Get the Complete Carpal Tunnel Recovery Guide — Same System That Helped Thousands
40+ pages of exercises, protocols, and the complete recovery plan. Instant download, 30-day money-back guarantee.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee