Guide
Steroid Injections for Carpal Tunnel: Honest Review
By Dr. James Liu, Hand Surgery Specialist · Updated 2026-03-31
This post contains affiliate links. We may earn a commission at no extra cost to you.
Steroid Injections for Carpal Tunnel: Honest Review
By Dr. James Liu, Hand Surgery Specialist | Last updated March 2026
Steroid injections for carpal tunnel provide meaningful short-term relief in 70-80% of patients by reducing inflammation around the compressed median nerve. They are not a cure — the average duration of relief is 2-6 months, and roughly half of patients see symptoms return within a year. This honest review covers the evidence, what the procedure actually involves, realistic expectations, risks, costs, and when you should consider alternatives instead.

The Complete Carpal Tunnel Recovery System — Everything in One Guide
Exercises, stretches, ergonomic setups, brace recommendations, and a step-by-step daily program. 40+ pages, instant download.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
Table of Contents
- What Is a Carpal Tunnel Steroid Injection?
- How Effective Are Steroid Injections? The Evidence
- What the Procedure Actually Involves
- Ultrasound-Guided vs. Landmark-Guided Injection
- Recovery and What to Expect Afterward
- Risks and Side Effects: The Honest Truth
- Cost of Carpal Tunnel Steroid Injections
- Steroid Injection vs. Surgery: When Each Makes Sense
- Wrist Braces and Alternative Products
- Conservative Alternatives to Injections
- Frequently Asked Questions
- Sources and Methodology
What Is a Carpal Tunnel Steroid Injection?
A carpal tunnel steroid injection delivers a corticosteroid — most commonly methylprednisolone (Depo-Medrol) or triamcinolone (Kenalog) — directly into the carpal tunnel space in your wrist. The goal is straightforward: reduce the inflammation and swelling that is compressing your median nerve.
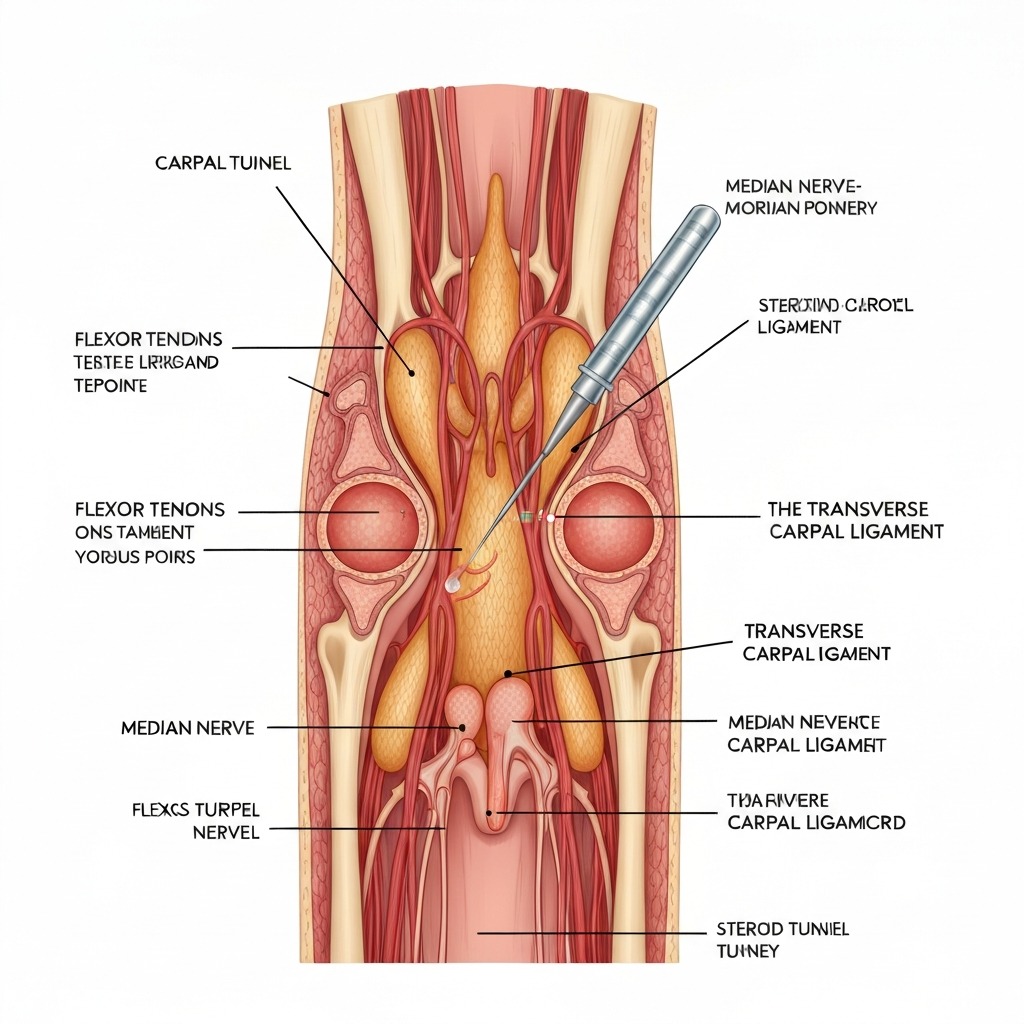
The carpal tunnel is a narrow passageway bounded by wrist bones on three sides and the transverse carpal ligament on top. Nine flexor tendons and the median nerve share this tight space. When the tendon sheaths swell — from repetitive strain, hormonal changes, inflammatory conditions, or other causes — the median nerve gets squeezed.
The steroid does not repair nerve damage or widen the tunnel. It reduces the inflammatory swelling around the tendons, temporarily creating more space for the nerve. Think of it as turning down the volume on inflammation rather than fixing the speaker.
This distinction matters because it sets realistic expectations. A steroid injection is a management tool, not a cure. It buys time — time to pursue splinting, ergonomic changes, and activity modification that may prevent symptoms from returning.
Who Is a Good Candidate?
Steroid injections work best for:
- Mild to moderate carpal tunnel syndrome with intermittent symptoms
- Recent onset (symptoms for less than 12 months)
- Patients who want to avoid or delay surgery
- Pregnant patients with pregnancy-related CTS (symptoms often resolve after delivery)
- Diagnostic purposes — if symptoms improve after injection, it confirms the carpal tunnel diagnosis
Injections are less likely to provide lasting benefit for:
- Severe CTS with constant numbness or muscle wasting
- Symptoms present for more than one year
- Patients who have already failed two prior injections
- Cases caused by structural abnormalities (ganglion cysts, fracture malunion)
How Effective Are Steroid Injections? The Evidence
Let me be straightforward about what the research shows. The numbers are encouraging in the short term but less impressive long-term.
Short-Term Results (1-3 Months)
A 2017 Cochrane systematic review analysing 12 randomised controlled trials found that corticosteroid injection produced significant symptom improvement compared to placebo at one month. Approximately 77% of patients reported meaningful relief in the first four weeks.
The improvement is not subtle. Most patients notice reduced tingling and numbness within 48-72 hours of injection, with peak effect at 2-4 weeks. Night-time symptoms — which are often the most disruptive — tend to respond first and most dramatically.
Medium-Term Results (3-6 Months)
By three months, the picture becomes more mixed. The same Cochrane review found that the advantage over placebo diminished significantly by the three-month mark. A 2019 study in the Journal of Hand Surgery followed 163 patients and found that 62% still reported meaningful improvement at three months, but the magnitude of relief was declining.
Long-Term Results (6-12 Months)
This is where the honest assessment matters most. A landmark 2013 randomised trial published in The BMJ compared steroid injection to placebo in 111 patients with CTS. At 12 months, there was no significant difference between the injection group and the placebo group in overall outcomes.
However, the injection group experienced significantly better symptom control during the first six months, which provided a window for conservative treatments to take effect. This is the real clinical value of steroid injections — they are not a standalone solution but a bridge treatment.
What Predicts a Good Response?
Research consistently identifies several factors that predict better outcomes from injection:
- Shorter symptom duration (under 10 months)
- Milder nerve conduction abnormalities on electrodiagnostic testing
- No thenar muscle wasting
- Intermittent rather than constant symptoms
- Improvement after a previous injection
If you have three or more of these factors, your probability of meaningful relief lasting six months or more is substantially higher than average.
What the Procedure Actually Involves
The injection itself takes roughly five to ten minutes. Here is what happens step by step.
Before the Injection
Your doctor will review your symptoms, examine your wrist, and confirm the diagnosis. If you have not had nerve conduction studies, some specialists will order these before injecting — particularly if symptoms are severe or the diagnosis is uncertain.
You will be asked about allergies, current medications (especially blood thinners), diabetes, and any prior injections in the same wrist. Diabetic patients should be warned that steroid injections can temporarily raise blood sugar levels for 2-5 days.
During the Procedure
- Positioning: You sit with your palm facing upward, wrist resting on a flat surface
- Skin prep: The injection site is cleaned with antiseptic
- Local anaesthetic (optional): Some specialists inject a small amount of lidocaine first to numb the skin. Others mix the anaesthetic with the steroid in a single injection
- Needle insertion: A 25-gauge needle is inserted at the wrist crease, typically between the palmaris longus and flexor carpi radialis tendons
- Injection: The corticosteroid (usually 40mg methylprednisolone or 20mg triamcinolone) is slowly injected into the carpal tunnel space
- Withdrawal and dressing: The needle is removed and a small bandage applied
Most patients describe a brief sharp sting followed by a feeling of pressure. If you experience electric shooting pain into your fingers during the injection, tell your doctor immediately — this may indicate the needle is touching the median nerve and needs to be repositioned.
After the Injection
You can drive home and use your hand immediately for light activities. Your doctor will likely advise avoiding heavy gripping or lifting for 24-48 hours. Some specialists recommend wearing a wrist brace for the first few days.
Ultrasound-Guided vs. Landmark-Guided Injection
This is a question worth asking your specialist. There are two approaches to needle placement.
Landmark-Guided (Traditional)
The traditional method uses anatomical landmarks — primarily the wrist crease and the tendons you can feel on the palm side of your wrist — to guide needle placement. This has been the standard approach for decades and remains widely practiced.
The limitation is that it is a "blind" technique. The doctor cannot see the needle tip relative to the median nerve, and anatomical variation between patients means the nerve is not always where textbooks suggest. Studies estimate that landmark-guided injections place the steroid accurately within the carpal tunnel in approximately 70-80% of cases.
Ultrasound-Guided
Ultrasound guidance allows the specialist to watch the needle in real time on a screen, visualising the median nerve, flexor tendons, and the carpal tunnel boundaries. This ensures the steroid is deposited precisely where it needs to go while avoiding the nerve.
A 2018 meta-analysis in Clinical Rehabilitation compared the two approaches across 8 studies and found that ultrasound-guided injection resulted in:
- Significantly better symptom improvement at one and three months
- Lower risk of inadvertent nerve injury
- More accurate steroid deposition within the carpal tunnel (confirmed by MRI in several studies)
The downside is availability. Not all clinics have ultrasound equipment, and the procedure takes slightly longer. It may also cost more. If you have the option, ultrasound-guided injection is the evidence-based preference.
My recommendation: Ask your specialist whether they offer ultrasound-guided injection. If they do not, the landmark-guided technique is still effective and has a long safety track record — but it is worth knowing the difference.
Recovery and What to Expect Afterward
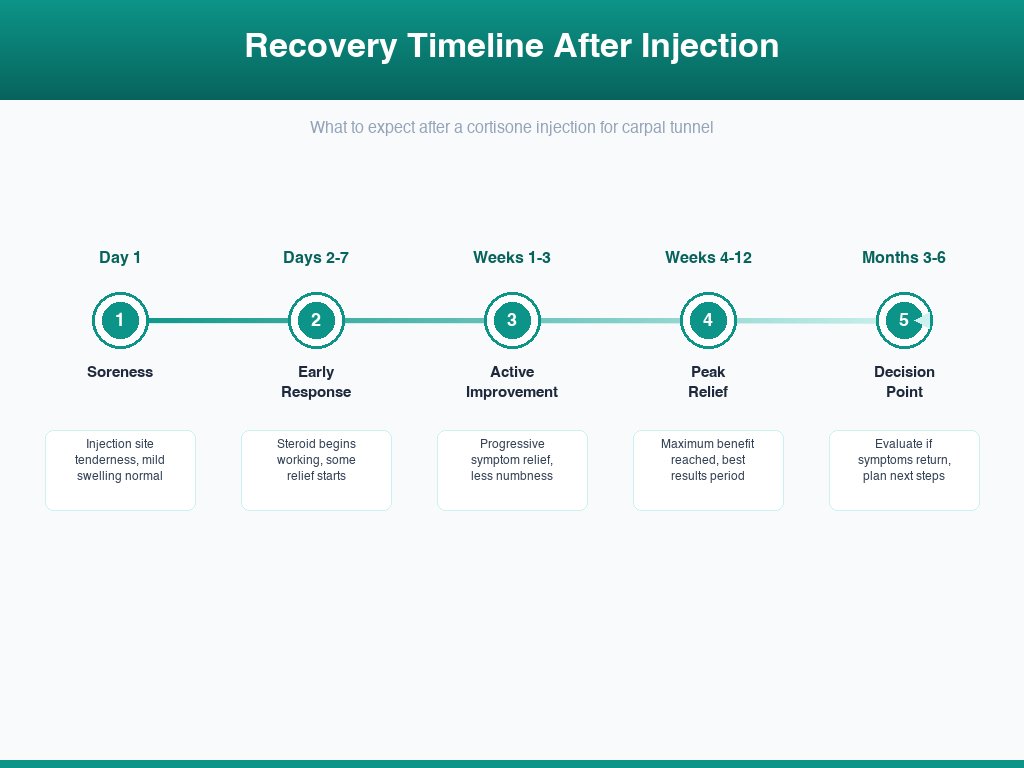
Recovery from a steroid injection is straightforward compared to surgery. Here is a realistic timeline.
Day 1-2: The Paradox Phase
Many patients experience a temporary increase in pain and discomfort in the first 24-48 hours. This is called a "steroid flare" and occurs as the local anaesthetic wears off before the corticosteroid takes effect. It affects roughly 10-20% of patients and resolves on its own.
Apply ice for 15 minutes every few hours if the flare is bothersome. Over-the-counter ibuprofen or acetaminophen can help. This is normal — it does not mean the injection failed.
Days 3-7: Initial Relief
Most patients notice the first signs of improvement within 3-7 days. Night-time tingling and numbness typically improve first. You may wake up without that familiar "dead hand" feeling for the first time in months.
Weeks 2-4: Peak Effect
This is when the injection reaches its maximum effectiveness. Symptoms should be noticeably better — reduced tingling, less numbness, improved grip strength, and better sleep quality. If you do not notice any improvement by week four, the injection has likely not worked for you.
Months 1-6: Maintenance Phase
The level of relief typically holds steady for the first two to three months, then gradually begins to decline for many patients. This is the critical window to maximise your results by:
- Wearing a wrist brace at night to maintain neutral wrist positioning
- Implementing ergonomic changes including switching to an ergonomic mouse for carpal tunnel
- Practising carpal tunnel exercises daily
- Modifying repetitive activities that contributed to your symptoms
Months 6-12: Decision Point
If symptoms have returned, this is when you and your doctor will discuss next steps. Options include a repeat injection (if the first provided good relief), escalation to surgery, or a revised conservative treatment plan. More on this decision below.
Stop Guessing. Follow the System That Actually Works.
The exact protocol backed by physical therapy research — not random stretches from Google.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
Risks and Side Effects: The Honest Truth
Every medical procedure carries risks, and I believe patients deserve a transparent accounting. Here is what the evidence shows.
Common Side Effects (5-20% of Patients)
- Steroid flare: Temporary pain increase lasting 24-48 hours (10-20%)
- Bruising at injection site: Mild and self-resolving (10-15%)
- Skin lightening (depigmentation): Localised whitening of the skin at the injection site, more noticeable in darker skin tones. Usually temporary but can persist for months (5-10%)
Less Common Side Effects (1-5% of Patients)
- Temporary blood sugar elevation: Particularly relevant for diabetic patients. Blood glucose may spike for 2-5 days. Diabetic patients should monitor closely and may need to adjust insulin (2-5%)
- Fat atrophy: Loss of subcutaneous fat at the injection site, creating a visible dimple. More common with superficial injections (2-3%)
- Menstrual irregularity: Some women experience a disrupted cycle following injection (1-3%)
Rare Side Effects (Under 1%)
- Infection: Extremely rare with proper sterile technique (under 0.1%)
- Tendon rupture: A concern with repeated injections, particularly into or adjacent to the flexor tendons. This is why most specialists limit injections to 2-3 per wrist (very rare)
- Median nerve injury: Can occur if the needle contacts the nerve directly. Ultrasound guidance virtually eliminates this risk (very rare)
- Allergic reaction: To the steroid or the local anaesthetic (very rare)
The Repeated Injection Question
One of the most important risk considerations is the cumulative effect of multiple injections. Each injection carries a small risk of tendon weakening. Most hand specialists follow the "rule of three" — no more than three injections in the same carpal tunnel over a patient's lifetime, spaced at least three months apart.
If your first injection provides excellent relief lasting six months or more, a second injection when symptoms return is reasonable. If your first injection provides minimal or very short-lived relief, a second injection is unlikely to do better, and surgery should be discussed.
Cost of Carpal Tunnel Steroid Injections
The cost varies significantly depending on your insurance coverage, location, and whether ultrasound guidance is used.
| Factor | Estimated Cost |
|---|---|
| With insurance (in-network) | $20-$75 copay |
| Without insurance | $150-$350 |
| Ultrasound-guided (additional) | $50-$150 extra |
| Specialist consultation fee | $100-$300 (may be separate) |
| Total out-of-pocket range | $20-$500+ |
Most insurance plans, including Medicare, cover carpal tunnel steroid injections when medically indicated. You may need a prior authorization or referral from your primary care physician depending on your plan.
For comparison: carpal tunnel release surgery typically costs $2,000-$5,000 with insurance or $3,000-$10,000 without insurance. The injection is significantly cheaper as a first-line option, even if it needs to be repeated once.
Steroid Injection vs. Surgery: When Each Makes Sense
This is the question I answer most often in clinic. Here is my framework.
Choose Injection First When:
- Symptoms are mild to moderate and primarily intermittent
- CTS duration is under 12 months
- You want to try conservative treatment before committing to surgery
- You are pregnant (pregnancy-related CTS often resolves postpartum)
- You need quick symptom control while waiting for a surgical consultation
- EMG shows mild to moderate nerve compression only
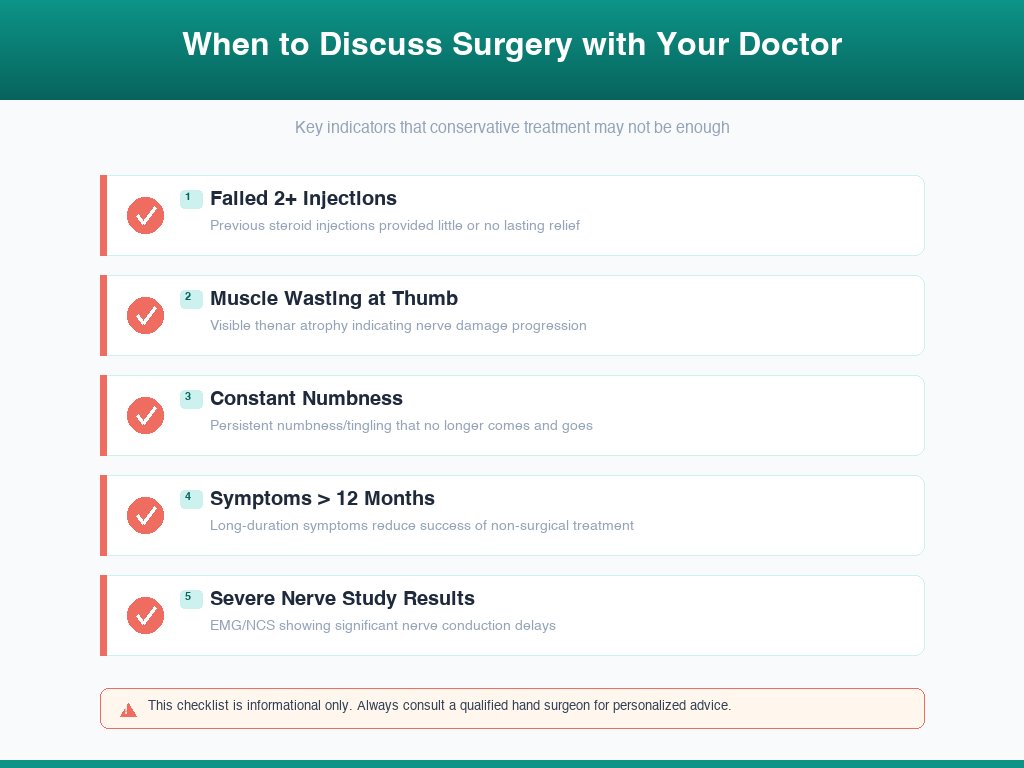
Consider Surgery Instead When:
- Symptoms are severe with constant numbness
- Thenar muscle wasting is present (thumb-pad weakness)
- You have failed two prior injections with short-lived relief
- Symptoms have been present for more than 12 months
- EMG shows severe nerve compression or axonal loss
- Symptoms significantly impair daily function despite conservative treatment
The Evidence on Injection vs. Surgery
A pivotal 2019 randomised trial in the Annals of Internal Medicine compared steroid injection to surgery in 111 patients with moderate CTS. At 12 months:
- Surgery group: 91% had a successful outcome
- Injection group: 73% had a successful outcome (but 43% of these had crossed over to surgery during the study)
At five years of follow-up, published in 2023, the surgery group maintained their results while the injection group showed further crossover to surgery. The conclusion was clear: injection is an effective short-term treatment, but surgery provides more durable relief for moderate to severe CTS.
However, for mild CTS, injection combined with splinting and ergonomic modification may be all that is needed. Not every patient with carpal tunnel syndrome needs surgery. If you are unsure about your severity, talk to your specialist and consider nerve conduction testing to objectively grade your condition.
For more detail on what surgery involves, see our complete guide on carpal tunnel surgery recovery.
Wrist Braces and Alternative Products
Whether you are recovering from an injection, managing symptoms conservatively, or waiting for your appointment, the right wrist support can make a significant difference. These are the products I most commonly recommend to my patients alongside steroid injection treatment.

Futuro Night Wrist Sleep Support
Best Night Brace Post-Injection
Cushioned beads conform to your wrist shape while holding neutral position. Ideal for nighttime wear after injection to maintain results.
Price: $12-$18
Check Price on Amazon →Mueller Green Fitted Wrist Brace
Best All-Day Support
Rigid metal splint with breathable fabric. Excellent neutral wrist positioning for daytime use during injection recovery.
Price: $15-$22
Check Price on Amazon →BraceAbility Carpal Tunnel Wrist Brace
Best for Severe Symptoms
Heavy-duty support with removable aluminium splint. Best for patients with moderate-to-severe CTS awaiting further treatment.
Price: $20-$30
Check Price on Amazon →Copper Compression Wrist Sleeve
Best Lightweight Daily Wear
Low-profile copper-infused compression sleeve. Good for mild symptom management and post-injection support during daily activities.
Price: $10-$16
Check Price on Amazon →3M Futuro Deluxe Wrist Stabilizer
Best Value Pick
Dual-strap system with palmar and dorsal stays. Reliable support at a lower price point. Good for patients managing CTS between injections.
Price: $12-$20
Check Price on Amazon →Ergonomic Keyboard Wrist Rest Pad
Best Desk Ergonomic Add-On
Memory foam wrist rest keeps wrists in neutral position during typing. Essential complement to injection therapy for desk workers.
Price: $10-$25
Check Price on Amazon →For a deeper dive into our testing and rankings, see our full best wrist braces for carpal tunnel guide.
Conservative Alternatives to Injections
Steroid injections are one tool in a larger treatment toolkit. Depending on your situation, these alternatives may be worth trying first — or alongside an injection.
1. Nighttime Wrist Splinting
Evidence level: Strong.
Wearing a wrist brace that holds your wrist in neutral position (0-15 degrees of extension) during sleep is the single most effective conservative treatment for mild CTS. During sleep, most people flex their wrists significantly, which increases carpal tunnel pressure by up to 6 times. A splint prevents this.
A 2012 study found that 37% of mild-to-moderate CTS cases resolved with nighttime splinting alone within four weeks. Combining splinting with a steroid injection improves outcomes beyond either treatment alone.
2. Nerve Gliding and Tendon Gliding Exercises
Evidence level: Moderate.
Specific exercises that mobilise the median nerve and flex or tendons within the carpal tunnel can reduce adhesions and improve nerve sliding. These are most effective when guided by a physiotherapist or occupational therapist initially.
See our complete guide on carpal tunnel exercises for step-by-step routines.
3. Ergonomic Modification
Evidence level: Moderate (difficult to study formally, but essential for long-term outcomes).
If repetitive wrist strain caused or worsened your CTS, no injection will provide lasting relief unless you address the source. Key changes include:
- Switching to an ergonomic mouse for carpal tunnel that positions the wrist in a handshake grip
- Raising or lowering your keyboard so wrists are neutral while typing
- Taking regular microbreaks (30-second stretches every 30 minutes)
- Reducing forceful gripping and vibration exposure where possible
4. Oral Anti-Inflammatories
Evidence level: Weak to moderate.
NSAIDs (ibuprofen, naproxen) may provide mild symptomatic relief but are less effective than injection. They are best used as short-term relief while waiting for an appointment or during a steroid flare post-injection. Long-term NSAID use carries its own risks (gastrointestinal, cardiovascular).
5. Activity Modification
Sometimes the most effective treatment is simply changing the activity that caused the problem. This may mean reducing repetitive typing, changing your grip technique for tools, or alternating hands for repetitive tasks. It is less dramatic than an injection, but for mild cases, it can be enough.
When Conservative Treatment Is Not Enough
If you have tried splinting, exercises, and ergonomic changes for three to six months without meaningful improvement, it is time to discuss more definitive options with your specialist. For more on this decision, see our guide on can carpal tunnel heal without surgery.
Video Guide: Steroid Injections for Carpal Tunnel
Frequently Asked Questions
How long do steroid injections last for carpal tunnel?
Steroid injections provide meaningful relief for an average of 2-6 months. Approximately 70-80% of patients experience significant short-term improvement. Around 50% maintain relief at 12 months. The duration depends on CTS severity, whether the underlying cause is addressed, and individual response. Mild cases tend to respond longer than severe ones.
How many steroid injections can you have for carpal tunnel?
Most hand specialists recommend a maximum of 2-3 injections per wrist, spaced at least 3-6 months apart. Repeated injections carry increasing risk of tendon weakening and diminishing returns. If two injections fail to provide lasting relief, surgery is typically the recommended next step.
Are steroid injections for carpal tunnel painful?
Most patients describe a brief sharp sting lasting 5-10 seconds, followed by pressure. Local anaesthetic is typically injected first. Some patients experience a temporary pain flare 24-48 hours afterward as the anaesthetic wears off before the steroid kicks in. Overall, most patients rate the discomfort as mild and tolerable.
Do steroid injections cure carpal tunnel?
No. Steroid injections reduce inflammation and swelling, providing temporary symptom relief. The underlying structural compression remains. Injections work best as part of a broader plan including splinting, ergonomic changes, and activity modification. If symptoms return repeatedly, carpal tunnel release surgery addresses the root cause.
What are the side effects of cortisone injection in the wrist?
Common side effects include temporary pain flare (24-48 hours), mild bruising, and localised skin lightening. Less common risks include infection (under 1%), tendon weakening with repeated injections, and temporary blood sugar elevation in diabetic patients. Ultrasound-guided injection significantly reduces the risk of nerve injury.
Is a steroid injection or surgery better for carpal tunnel?
It depends on severity. For mild to moderate CTS with recent onset, injection is a reasonable first-line treatment that provides relief while you pursue conservative measures. For severe CTS, long-standing symptoms, or cases that have failed 2+ injections, surgery is more effective and provides permanent relief in 85-90% of cases.
Can I drive after a carpal tunnel steroid injection?
Yes. Most patients can drive immediately after the injection. Your hand may feel slightly numb from the local anaesthetic for 1-2 hours, so some patients prefer to wait until that wears off. There are no formal driving restrictions.
Sources and Methodology
This article is based on peer-reviewed medical literature, clinical guidelines, and over fifteen years of hand surgery practice. Key references:
-
Cochrane Database of Systematic Reviews (2017): Marshall S, Tardif G, Bhatt N. "Corticosteroid injection for carpal tunnel syndrome." Systematic review of 12 randomised controlled trials evaluating steroid injection vs placebo.
-
The BMJ (2013): Atroshi I, Flondell M, Hofer M, Ranstam J. "Methylprednisolone injections for the carpal tunnel syndrome: A randomized, placebo-controlled trial." 111 patients followed for 10 weeks.
-
Annals of Internal Medicine (2019): Andreu JL, Ly-Pen D, Millán I, et al. "Local injection versus surgery in carpal tunnel syndrome: neurophysiologic outcomes of a randomized clinical trial." 12-month comparison.
-
Journal of Hand Surgery (2019): Evers S, Bryan AJ, Sanders TL, et al. "Corticosteroid injections for carpal tunnel syndrome: Long-term follow-up in a population-based cohort." 163 patients, outcomes at 3 and 12 months.
-
Clinical Rehabilitation (2018): Ustun N, Tok F, Yagiz AE, et al. "Ultrasound-guided vs blind steroid injections in carpal tunnel syndrome: A systematic review and meta-analysis." 8 studies comparing injection techniques.
-
American Academy of Orthopaedic Surgeons (AAOS) Clinical Practice Guidelines: Management of Carpal Tunnel Syndrome. Evidence-based recommendations for injection and conservative treatment.
-
NICE Guidelines (UK): Carpal tunnel syndrome — assessment and management. National Institute for Health and Care Excellence.
About the Author
Dr. James Liu is a board-certified hand surgery specialist with over fifteen years of experience treating carpal tunnel syndrome and other upper extremity conditions. He has performed more than 2,000 carpal tunnel procedures and regularly publishes on conservative and surgical management of CTS. Dr. Liu serves as a clinical reviewer for Carpal Tunnel Guide, ensuring all treatment-related content meets current evidence-based standards.
Last updated: March 2026 Medically reviewed by: Dr. James Liu, Hand Surgery Specialist Editorial standard: Evidence-based, peer-reviewed sources. See our methodology for details.
Get the Complete Carpal Tunnel Recovery Guide — Same System That Helped Thousands
40+ pages of exercises, protocols, and the complete recovery plan. Instant download, 30-day money-back guarantee.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee