Guide
Carpal Tunnel Surgery: What to Expect and Recovery Time
By Rachel Torres, Content Specialist · Updated 2026-03-21
Carpal tunnel release surgery severs the transverse carpal ligament to relieve pressure on the median nerve. Most patients see night-time pain and tingling resolve within days to weeks of surgery. Full recovery of grip strength and sensation takes 3-6 months, with the majority achieving good to excellent long-term outcomes.
By Rachel Torres, Content Specialist | Last updated: March 2026
The Complete Carpal Tunnel Recovery System — Everything in One Guide
Exercises, stretches, ergonomic setups, brace recommendations, and a step-by-step daily program. 40+ pages, instant download.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
Table of Contents
- When Surgery Is Recommended
- Types of Carpal Tunnel Surgery
- What Happens During the Procedure
- Carpal Tunnel Surgery Recovery Timeline
- What You Can and Cannot Do Post-Op
- Physical Therapy and Rehabilitation
- Managing Pain and Complications
- Long-Term Outcomes and Success Rates
- FAQ: Carpal Tunnel Surgery
- Sources and Methodology
When Surgery Is Recommended

Carpal tunnel surgery is not the first line of treatment. Most cases of carpal tunnel syndrome respond to conservative management — night splints, activity modification, corticosteroid injections, and ergonomic changes. Surgery is typically recommended when:
- Symptoms persist or worsen after 3-6 months of consistent conservative treatment
- Nerve conduction studies (NCS) or electromyography (EMG) confirm significant median nerve compression or early nerve damage
- Thenar muscle wasting is present — weakness or wasting of the thumb-base muscles indicates advanced compression requiring prompt surgical intervention
- Constant numbness (not just intermittent tingling) suggests chronic nerve damage that conservative treatment cannot reverse
- Severe functional impairment — inability to use the hand for daily activities, repeated dropping of objects, inability to perform work duties
It is important to understand that surgery works best before significant permanent nerve damage occurs. Long-standing, severe compression can result in irreversible changes that surgery cannot fully correct. Do not delay indefinitely if conservative treatment is not working.
The Role of Ergonomic Modifications Before Surgery
Before proceeding to surgery, a comprehensive trial of ergonomic intervention is worth completing. This includes reviewing your workstation setup, mouse type, and keyboard positioning. Many patients find that switching to a vertical mouse reduces wrist strain enough to delay or even avoid surgery — particularly in early to moderate cases where nerve damage has not yet occurred.
For wrist support during this trial period, see our best wrist braces for carpal tunnel 2026 guide. You can also check current wrist brace prices on Amazon for the latest options. Learning carpal tunnel exercises can also help reduce symptoms while awaiting surgery.
Types of Carpal Tunnel Surgery
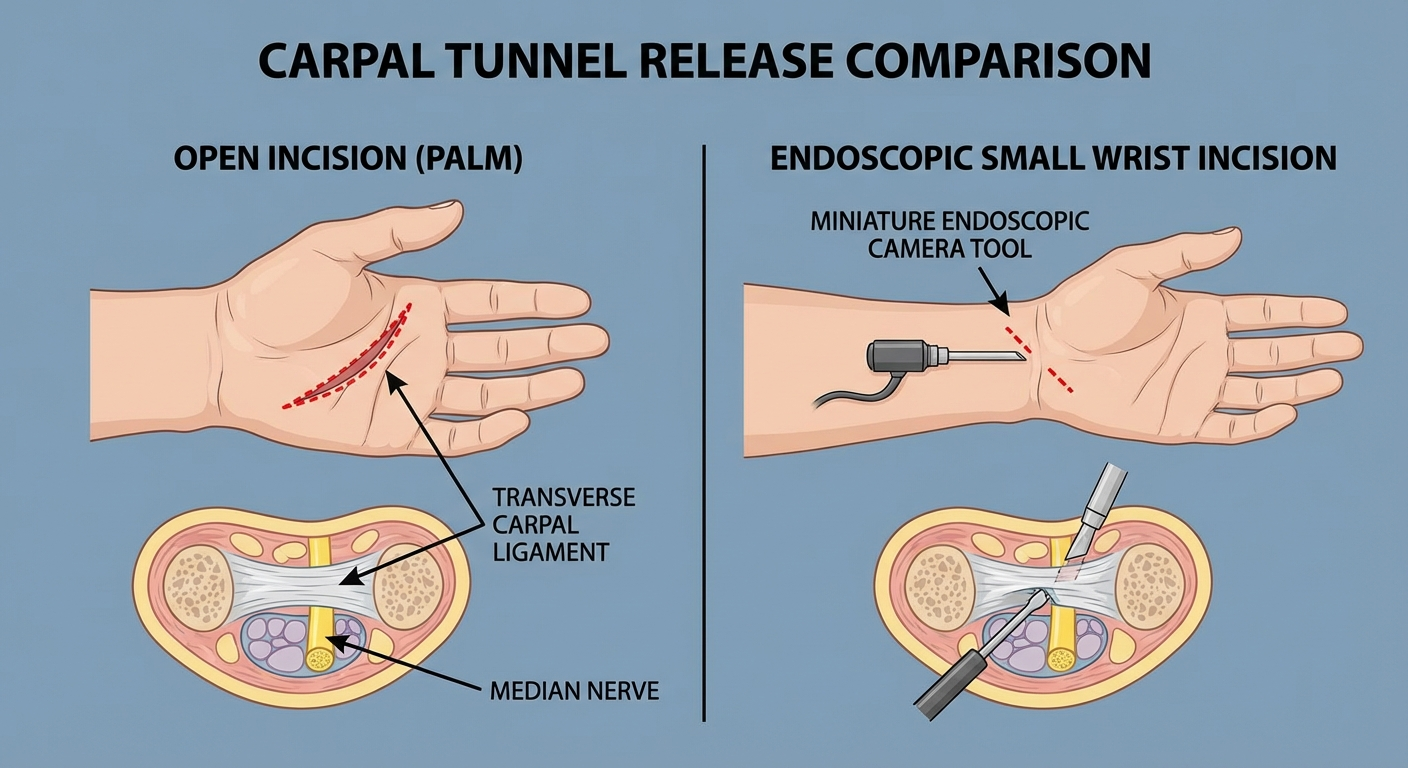
There are two main surgical approaches for carpal tunnel release. Both achieve the same goal — dividing the transverse carpal ligament to create more space for the median nerve — but through different access routes.
Open Carpal Tunnel Release (OCTR)
The traditional approach involves a 2-3 cm incision in the palm, typically running from the wrist crease toward the middle of the palm. The surgeon directly visualises and cuts the transverse carpal ligament under local anaesthesia.
Advantages:
- Widely performed — available at virtually all hand surgery centres
- Surgeon has direct visualisation of structures, reducing risk of accidental nerve or vessel damage
- Suitable for complex cases or patients with prior wrist surgery
- Lower cost than endoscopic in most settings
Disadvantages:
- Larger incision means more initial post-operative pain at the palm scar
- Longer time before full grip strength returns (scar tissue in the palm takes longer to mature)
- "Pillar pain" — soreness at the thenar and hypothenar eminences — is more common and can persist 3-6 months
Endoscopic Carpal Tunnel Release (ECTR)
One or two small incisions (5-10 mm each) are made at the wrist crease. A thin camera and cutting instrument are inserted. The surgeon views the ligament on a monitor and cuts it from the internal surface.
Advantages:
- Faster return to work and daily activities (typically 1-2 weeks sooner than open)
- Less post-operative palm scar tenderness
- Reduced pillar pain in most patients
- Smaller, less visible scars
Disadvantages:
- Requires a surgeon experienced specifically with endoscopic technique
- Less common than open — not available at all centres
- Marginally higher risk of incomplete ligament release or nerve injury in less experienced hands
- May not be appropriate for patients with prior wrist surgery or unusual anatomy
Long-Term Equivalence
Multiple systematic reviews confirm that open and endoscopic carpal tunnel release achieve equivalent outcomes at 1 year and beyond. The choice is primarily about short-term recovery speed versus procedure availability and surgeon expertise.
Open Release
- Incision: 2-3 cm palm
- Duration: 15-30 minutes
- Return to desk work: 4-6 weeks
- Full grip strength: 3-4 months
- Availability: Widely available
Endoscopic Release
- Incision: 1-2 small cuts (5mm)
- Duration: 20-40 minutes
- Return to desk work: 2-4 weeks
- Full grip strength: 2-3 months
- Availability: Specialist centres
What Happens During the Procedure
Understanding what happens during surgery reduces pre-operative anxiety and helps you prepare appropriately.
Pre-Operative Preparation
Most carpal tunnel surgery is performed as day surgery — you arrive, have the procedure, and go home the same day. In the week before surgery:
- Stop aspirin, ibuprofen, and other blood-thinning medications (your surgeon will specify timing)
- Arrange transport home — you cannot drive with a numb or bandaged hand
- Organise help for the first 2-3 days for cooking, dressing, and other two-hand tasks
- Prepare a comfortable recovery space with your wrist elevated on a pillow
Anaesthesia
Carpal tunnel release is almost universally performed under local anaesthesia with a tourniquet on the upper arm. You will be awake but feel no pain in the hand. Some centres offer a light sedative (twilight sedation) for anxious patients, but this is not typically necessary.
A Bier block (intravenous regional anaesthesia) is occasionally used for endoscopic procedures. General anaesthesia is rarely needed or recommended for this procedure.
The Procedure Itself
Open release (approximately 15-30 minutes):
- The skin is cleaned and draped. Local anaesthetic is injected.
- The tourniquet is inflated to provide a bloodless surgical field.
- The surgeon makes the palm incision and carefully dissects through skin and fat.
- The transverse carpal ligament is identified and divided under direct vision.
- The median nerve and surrounding structures are inspected.
- The wound is irrigated, the tourniquet deflated, and bleeding points controlled.
- The skin is closed with sutures and dressed with a padded bandage.
Endoscopic release (approximately 20-40 minutes):
- Similar preparation to open release.
- One or two small incisions at the wrist (and sometimes palm).
- The endoscope is inserted and the carpal tunnel visualised on screen.
- A blade attachment cuts the ligament from below.
- The instruments are removed and incisions closed with 1-2 sutures.
Immediately Post-Procedure
You will spend 30-60 minutes in recovery. Your hand will be bandaged with the wrist in a neutral position. You should be able to move your fingers, though they may feel clumsy due to the bandaging and residual local anaesthetic. Pain as the anaesthetic wears off is typically mild to moderate — most patients describe it as 3-5/10.
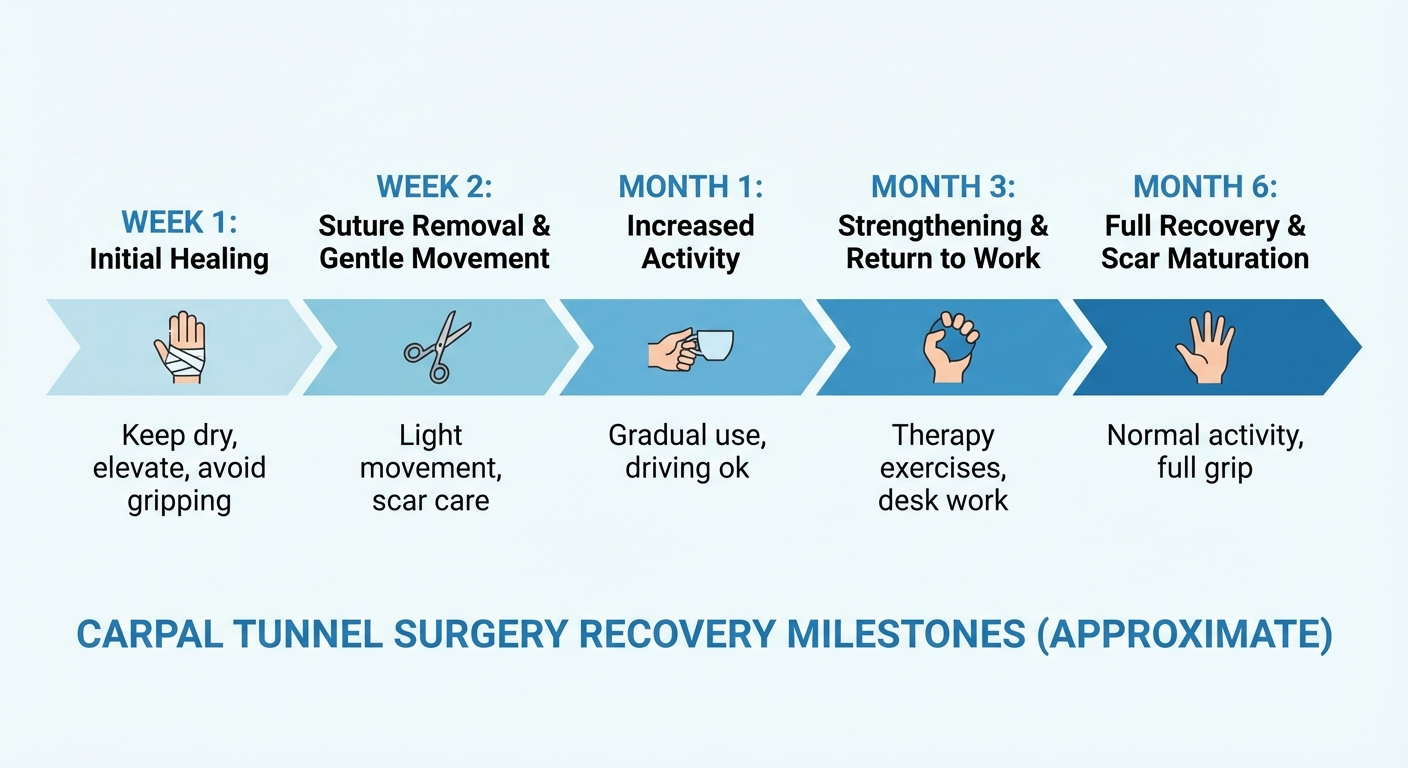
Carpal Tunnel Surgery Recovery Timeline

Recovery from carpal tunnel surgery follows a predictable but individual course. Here is what to expect at each stage.
Days 1-3: Immediate Post-Operative Period
- Symptom changes: Night-time pain and sleep disruption often improve dramatically within the first 24-48 hours — for many patients this is the most immediately obvious change
- Pain: Mild to moderate, manageable with over-the-counter analgesics (paracetamol, ibuprofen if permitted). Ice wrapped in a cloth applied 20 minutes on/off helps.
- Numbness and tingling: Typically unchanged or slightly worse in the first few days as the nerve "wakes up"
- Activity: Rest the hand. Keep it elevated above heart level when sitting or lying down. Finger movement is encouraged — gently flex and extend all fingers several times per hour to prevent stiffness.
- Wound care: Keep the dressing dry and intact. No shower unless you waterproof the bandage.
Week 1-2: Early Recovery
- Dressing review: A wound check at 7-14 days depending on your surgical centre. Sutures may be removed at this appointment (some use dissolvable sutures).
- Hand use: Light finger use for tasks like eating, using a phone, turning pages. No gripping, pinching, or lifting.
- Driving: Not yet — most surgeons clear driving at 2-4 weeks depending on which hand was operated and your vehicle (automatic vs manual).
- Return to office work: Typically not yet recommended — wound healing and dressing limit computer use.
- Sensory improvement: Many patients notice early improvement in tingling during this period as nerve inflammation subsides.
Weeks 2-4: Early Mobilisation
- Sutures out: If not already removed, dissolvable sutures will have dissolved.
- Scar management: Begin gentle scar massage with a neutral moisturiser (vitamin E cream or similar) 2-3 times daily once wound is fully closed. This reduces scar tethering and pillar pain.
- Activity: Begin progressive light use — writing, typing with minimal pressure, light food preparation. Still avoid heavy gripping.
- Return to desk/computer work: Most non-manual workers can return to office work in weeks 2-4, using an ergonomic setup with wrist support. A vertical mouse reduces wrist strain significantly during this return-to-work period. In fact, after recovery, switching to an ergonomic vertical mouse prevents recurrence — it is one of the most evidence-based ergonomic changes you can make.
- Driving: Typically cleared for automatic vehicles at this stage if grip is sufficient to steer safely.
Weeks 4-8: Progressive Return to Activity
- Grip strength: Still significantly below pre-operative level. Normal grip recovery takes longer with open release than endoscopic.
- Occupational therapy: If you are working in a manual role, hand therapy should begin in this window.
- Pillar pain: Soreness at the base of the thumb and little finger is common and often peaks in weeks 3-6. It resolves on its own for the majority of patients.
- Sensory recovery: Tingling continues improving. Persistent numbness in the fingertips may remain for months if pre-operative nerve damage was significant.
- Return to light manual work: Typically by week 6-8 for most patients.
3-6 Months: Full Recovery
- Grip strength: Returns to near pre-operative levels by 3 months in most patients; full strength by 4-6 months.
- Scar maturation: The palm scar typically flattens and fades through this period. Scar massage and desensitisation exercises are important throughout.
- Heavy lifting and manual labour: Cleared by most surgeons at 3-4 months.
- Return to competitive sport: Usually cleared at 3-4 months depending on sport demands.
- Residual symptoms: A small percentage (5-15%) of patients have residual mild symptoms at 6 months, particularly if pre-operative nerve damage was severe. Most continue to improve slowly beyond 6 months.
Stop Guessing. Follow the System That Actually Works.
The exact protocol backed by physical therapy research — not random stretches from Google.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
What You Can and Cannot Do Post-Op

First 2 Weeks: Major Restrictions
❌ No lifting over 0.5-1 kg with the operated hand ❌ No gripping tools, jars, or heavy objects ❌ No submerging the hand in water (baths, swimming, dishwashing without waterproof protection) ❌ No driving ❌ No strenuous exercise affecting arm position or blood pressure
✅ Light finger movement and gentle range-of-motion exercises ✅ Typing with minimal pressure (brief periods) ✅ Using phone and light tasks ✅ Keeping hand elevated when resting
Weeks 2-6: Graduated Return
❌ No heavy manual work, power tools, or vibrating equipment ❌ No heavy gripping or repetitive pinching ❌ No contact sports
✅ Progressive office work with ergonomic adaptations ✅ Light cooking and self-care ✅ Walking, stationary cycling (no handgrip cycling) ✅ Driving (cleared by surgeon, typically weeks 2-4)
Months 2-4: Near-Normal Activity
Most daily activities are possible by this stage. Continue avoiding: ❌ Heavy lifting over 5-10 kg with the operated hand ❌ Prolonged vibratory tool use (chainsaw, jackhammer)
When to Call Your Surgeon
Contact your surgical team promptly if you experience:
- Increasing redness, warmth, or swelling (wound infection signs)
- Wound edges opening or discharge
- Fever over 38°C/100.4°F
- Sudden severe pain not controlled by prescribed medications
- New or worsening numbness affecting the entire hand (rare but important)
Physical Therapy and Rehabilitation
Occupational therapy (hand therapy) significantly improves outcomes — particularly for patients with pre-operative muscle wasting, those returning to manual work, or anyone experiencing slow grip recovery.
When Therapy Begins
Early gentle range-of-motion exercises begin in the first week. Formal occupational therapy or hand therapy typically starts at 2-4 weeks post-op, once the wound is sufficiently healed.
What Hand Therapy Involves
Scar management: Silicone gel sheets, scar massage, desensitisation techniques. A well-managed scar is pliable, flat, and non-adherent to underlying structures — contributing to better long-term function.
Range-of-motion exercises: Wrist and finger mobility work to prevent stiffness from immobilisation and scar tethering.
Progressive strengthening: Starting with light putty exercises and advancing to functional resistance training over 8-12 weeks.
Sensory re-education: When significant sensory loss was present pre-operatively, graded sensory re-education helps the brain re-map nerve signals as they recover.
Work simulation: For patients returning to specific manual tasks, the therapist can simulate work demands and ensure safe return.
Managing Pain and Complications
Common Post-Operative Symptoms
Pillar pain is the most common post-operative complaint — a deep aching pain at the thenar eminence (thumb side) and/or hypothenar eminence (little finger side) of the palm. It affects up to 30% of open release patients and typically peaks at 3-6 weeks, resolving by 3-6 months. Scar massage, heat, and activity modification help. Rarely, persistent pillar pain requires steroid injection or scar release.
Scar tenderness at the palm incision is normal and improves with scar massage and desensitisation. A hypertrophic or thickened scar is uncommon but treatable with silicone sheets.
Prolonged numbness in the first few months is usually nerve recovery in progress. Nerves regenerate slowly — approximately 1 mm per day — so full sensory return after significant pre-operative damage may take 6-12 months.
Serious Complications (Uncommon)
Carpal tunnel release is among the safest surgical procedures. Serious complications are uncommon but include:
- Wound infection: Less than 1% of cases. Treated with antibiotics; rarely requires wound washout.
- Incomplete ligament release: Can occur, more commonly with endoscopic technique in inexperienced hands. May require revision surgery.
- Nerve or vessel injury: Rare (under 1%) in experienced hands. Typically the palmar cutaneous branch of the median nerve, causing a small area of numbness near the scar.
- Complex regional pain syndrome (CRPS): Very rare. Characterised by disproportionate pain, skin changes, and swelling. Requires specialist management.
Long-Term Outcomes and Success Rates

Carpal tunnel release has excellent long-term outcomes when performed appropriately.
What Surgery Reliably Improves
- Night-time pain and sleep disruption: resolves in most patients within days to weeks
- Intermittent tingling and electric sensations: typically resolves within weeks to months
- Grip strength: returns to near-normal in most patients by 3-6 months
- Patient satisfaction: 70-90% report good or excellent outcomes in long-term follow-up studies
What Surgery May Not Fully Reverse
- Long-standing thenar muscle wasting: Muscle atrophy present before surgery may partially but not fully recover, depending on severity
- Constant numbness from chronic nerve damage: Some residual sensory deficit may persist if pre-operative nerve damage was severe and prolonged
- Bilateral symptoms: If both hands are affected, the non-operated hand remains symptomatic until its own surgery
Factors Affecting Outcome
- Duration of symptoms before surgery: Earlier surgery generally produces better outcomes
- Age: Younger patients typically recover faster and more completely
- Pre-operative severity: Mild to moderate CTS has better surgical outcomes than severe
- Presence of comorbidities: Diabetes, thyroid disorders, and inflammatory arthritis can slow or limit recovery
- Surgeon experience: Outcomes are better at higher-volume centres


Recommended Recovery Products
These products support recovery and prevention after carpal tunnel surgery.
| Product | Purpose | When to Use | Buy |
|---|---|---|---|
| Post-Surgical Wrist Splint | Protect incision and reduce swelling | Days 1-14 | Check Amazon |
| Hand Grip Strengthener Set | Rebuild grip strength in Phase 3 | Weeks 4+ | Check Amazon |
| Therapy Putty Set | Fine motor rehab and scar mobilisation | Weeks 3-12 | Check Amazon |
| Wrist Ice/Heat Pack | Swelling management and stiffness relief | Throughout recovery | Check Amazon |
| Ergonomic Vertical Mouse | Prevent recurrence when returning to desk work | Week 2+ (when returning to computer) | Check Amazon |
For those comparing symptoms, our guide to carpal tunnel vs tendinitis covers the key differences to help confirm diagnosis.
FAQ: Carpal Tunnel Surgery
How long does carpal tunnel surgery recovery take? Full recovery takes 3-6 months. Most patients can do light daily activities within 2-4 weeks and return to desk work at 4-6 weeks. Manual labour clearance is typically at 3-4 months.
Is carpal tunnel surgery worth it? For moderate to severe CTS not responding to conservative treatment, surgery achieves good to excellent results in 70-90% of patients.
What is the difference between open and endoscopic carpal tunnel surgery? Both sever the same ligament. Open uses a 2-3 cm palm incision. Endoscopic uses tiny incisions and a camera. Endoscopic results in faster initial recovery; long-term outcomes are equivalent.
Can carpal tunnel come back after surgery? Recurrence rates are under 10% at 5 years. Recurrence is more likely if underlying causes (diabetes, arthritis, thyroid issues) are not addressed.
Do I need physical therapy after carpal tunnel surgery? Hand therapy is strongly recommended for patients with pre-operative muscle wasting, manual workers, or anyone with slow grip recovery. It significantly improves outcomes.
Sources and Methodology
-
Huisstede, B.M. et al. (2022). "Carpal Tunnel Syndrome: Hand Surgeons, Hand Therapists, and Physical Medicine and Rehabilitation Physicians Agree on a Multidisciplinary Treatment Guideline." Archives of Physical Medicine and Rehabilitation, 103(5), 1007-1015.
-
Scholten, R.J.P.M. et al. (2007). "Surgical Treatment Options for Carpal Tunnel Syndrome." Cochrane Database of Systematic Reviews. Meta-analysis comparing open versus endoscopic carpal tunnel release outcomes.
-
American Academy of Orthopaedic Surgeons (AAOS). (2023). Clinical Practice Guideline: Management of Carpal Tunnel Syndrome. Evidence-based treatment pathway including surgical indications.
-
Bland, J.D.P. (2007). "Carpal Tunnel Syndrome." BMJ, 335(7615), 343-346. Clinical overview of diagnosis and treatment including surgical management.
-
Thoma, A. et al. (2004). "A Meta-Analysis of Studies Comparing Open and Endoscopic Carpal Tunnel Decompression." Plastic and Reconstructive Surgery, 114(5), 1137-1146. Direct comparison of surgical technique outcomes.
-
National Institute for Health and Care Excellence (NICE). (2023). Carpal Tunnel Syndrome: Assessment and Treatment. UK clinical guideline for carpal tunnel management pathways.
-
Ibrahim, T. et al. (2009). "Pillar Pain After Open Carpal Tunnel Release: A Review." Journal of Hand Surgery, 34(3), 394-400. Specific evidence on pillar pain incidence and management.
Rachel Torres is a content specialist with expertise in musculoskeletal health and surgical recovery. She researches clinical evidence across orthopaedic and hand surgery literature to produce practical, accurate guidance for patients preparing for and recovering from upper limb procedures.
Get the Complete Carpal Tunnel Recovery Guide — Same System That Helped Thousands
40+ pages of exercises, protocols, and the complete recovery plan. Instant download, 30-day money-back guarantee.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee