Guide
Steroid Injections for Carpal Tunnel: An Honest Review (2026)
By Rachel · Updated 2026-04-27
Corticosteroid injections into the carpal tunnel reduce inflammation around the median nerve, providing relief for 70-80% of patients with mild to moderate carpal tunnel syndrome. The relief is real — but for most people, it is temporary, lasting weeks to months rather than years. Here is what the evidence actually says, what the procedure is like, and whether it is the right choice for you.
By Rachel Torres, Content Specialist | Last updated: April 2026
The Complete Carpal Tunnel Recovery System — Everything in One Guide
Exercises, stretches, ergonomic setups, brace recommendations, and a step-by-step daily program. 40+ pages, instant download.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
Table of Contents
- What Is a Steroid Injection for Carpal Tunnel?
- How Do Corticosteroid Injections Work?
- Who Is a Good Candidate?
- The Injection Procedure: What to Expect
- Effectiveness Rates: What the Research Says
- How Long Does Relief Last?
- Side Effects and Risks
- Cost and Insurance Coverage
- Recovery After the Injection
- Steroid Injections vs Other Treatments
- FAQ: Steroid Injections for Carpal Tunnel
- Sources and Methodology
What Is a Steroid Injection for Carpal Tunnel?
A corticosteroid injection for carpal tunnel syndrome is a minimally invasive procedure in which a anti-inflammatory steroid medication — most commonly triamcinolone acetonide, methylprednisolone, or dexamethasone — is injected directly into the carpal tunnel of the wrist. The goal is to reduce inflammation and swelling of the tissues surrounding the median nerve, thereby reducing nerve compression and relieving the pain, numbness, and tingling that define carpal tunnel syndrome.
This is not the same as a topical steroid cream or an oral steroid taper. The injection delivers a concentrated dose of anti-inflammatory medication precisely where it is needed, at the site of the problem. Because the carpal tunnel is a confined space with limited capacity, even a small volume of steroid can achieve a meaningful reduction in pressure on the nerve.
The procedure is typically performed in an outpatient setting — a GP's surgery, an orthopaedic clinic, or a hand therapy specialist's rooms. It takes less than five minutes, requires no sedation, and most patients drive themselves home afterwards.
Corticosteroid injections are considered a first-line conservative treatment for carpal tunnel syndrome, sitting alongside wrist splinting and ergonomic modification. They are also used as a diagnostic tool: if symptoms improve significantly after the injection, it strongly supports a diagnosis of carpal tunnel syndrome and helps rule out other causes of hand and wrist pain.
How Do Corticosteroid Injections Work?

To understand why steroid injections work, it helps to understand what is actually happening inside a wrist with carpal tunnel syndrome.
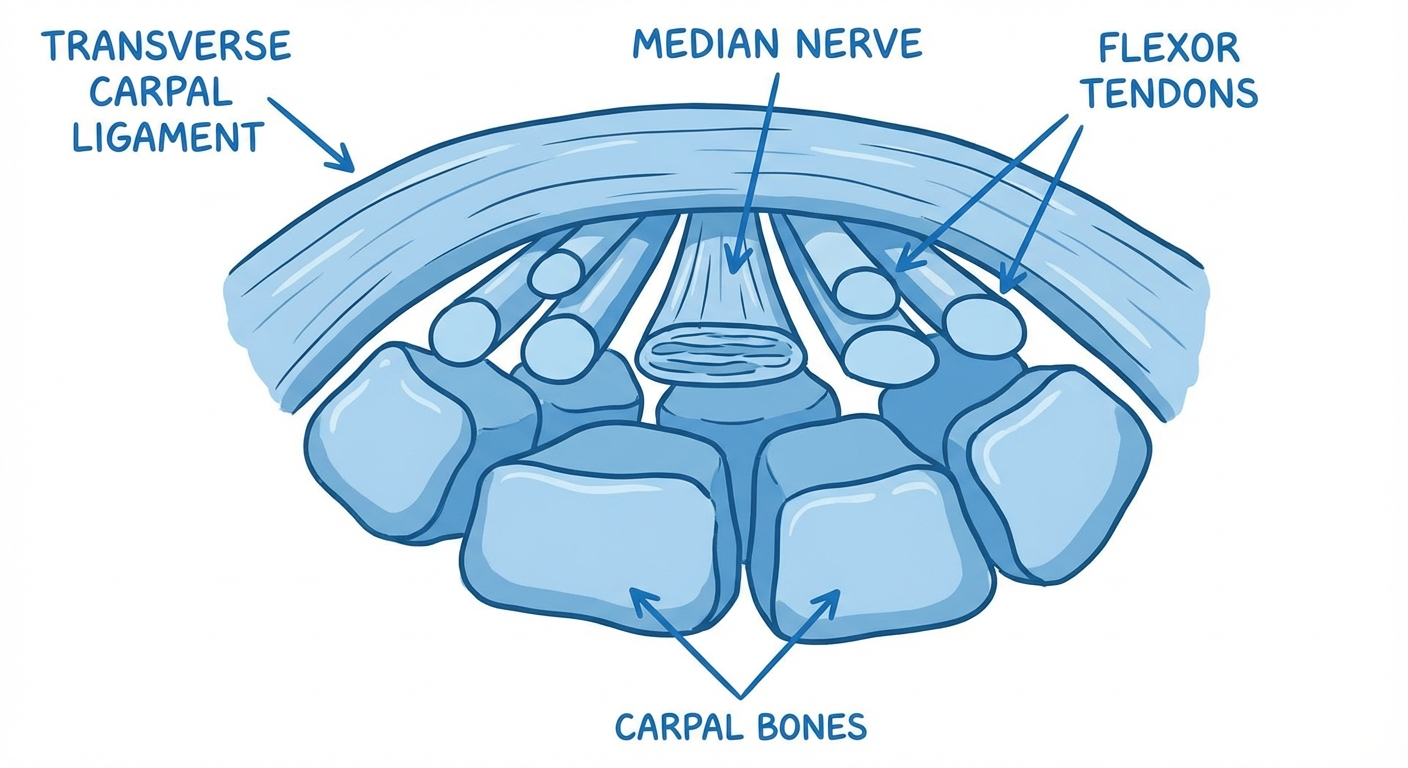
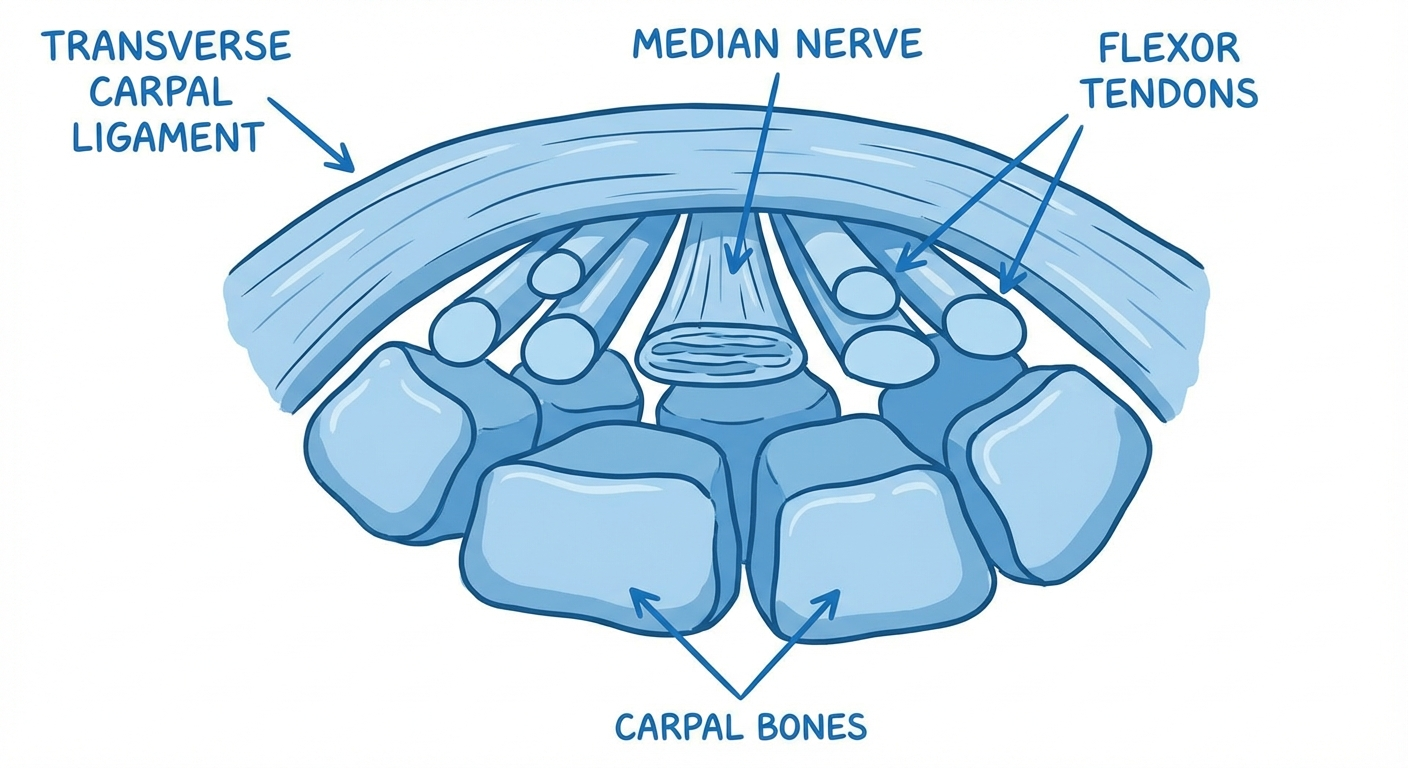
The carpal tunnel is a narrow passage on the palm side of the wrist, formed by the carpal bones below and the transverse carpal ligament above. Through this tunnel pass the median nerve and nine flexor tendons. When the tissues lining these tendons swell — due to repetitive strain, fluid retention, inflammatory conditions, pregnancy, or idiopathic causes — pressure inside the tunnel increases. The median nerve, which is the softest structure in the tunnel, bears the brunt of this pressure.
The resulting compression impairs the nerve's blood supply and disrupts its electrical signalling, producing the characteristic symptoms of carpal tunnel syndrome: numbness, tingling, burning, and electric shock sensations in the thumb, index, middle, and ring fingers; weakness in thumb grip; and pain radiating up the forearm.
Corticosteroids are synthetic versions of the hormones produced by the adrenal cortex. When delivered as an injection into the carpal tunnel, they work through two primary mechanisms:
-
Potent anti-inflammatory action — Steroids suppress the production of inflammatory chemicals (prostaglandins, cytokines, and leukotrienes) by binding to glucocorticoid receptors in inflamed tissues. This reduces swelling of the tendon linings inside the tunnel, creating more room for the median nerve.
-
Direct nerve membrane effects — Corticosteroids also appear to have a direct stabilising effect on nerve cell membranes, reducing ectopic (abnormal) electrical firing that causes paraesthesia symptoms. This is separate from the anti-inflammatory effect and may explain why some patients feel relief even before the inflammation visibly subsides.
The steroid is typically combined with a small volume of local anaesthetic (such as lidocaine), which provides almost immediate — though temporary — numbness. Patients often notice relief within minutes of the injection as the anaesthetic takes effect, before the steroid has even begun to work. This anaesthetic effect fades within a few hours; the steroid's anti-inflammatory effect builds over 3-14 days.
Who Is a Good Candidate?

Not every person with carpal tunnel symptoms is an ideal candidate for an injection. Understanding who benefits most helps set realistic expectations.
Strong Candidates for Steroid Injection
Mild to moderate CTS — Patients with intermittent symptoms, no constant numbness, and confirmed median nerve compression on nerve conduction studies respond best. If you still have good grip strength and no visible muscle wasting at the thumb base, an injection is a very reasonable first-line option.
Pregnancy-related carpal tunnel syndrome — Hormonal changes during pregnancy cause fluid retention and tissue swelling that often triggers or worsens CTS. Pregnant patients are excellent candidates because the condition frequently resolves after delivery, and an injection avoids the need for oral medications. Wrist splinting at night combined with a steroid injection if needed is the standard approach during pregnancy.
Patients wanting to delay or avoid surgery — Some patients prefer to exhaust all conservative options before considering carpal tunnel release surgery. Steroid injections buy time and can provide meaningful relief for those not ready for a surgical decision.
Early-stage disease confirmed by electrodiagnostic testing — Nerve conduction studies (NCS) or electromyography (EMG) that show mild to moderate median nerve slowing — rather than severe conduction block — predict a better response to injections.
Patients with inflammatory conditions — Those with rheumatoid arthritis, psoriatic arthritis, or gout affecting the wrist tendons may have a particularly pronounced inflammatory component to their CTS, which responds well to steroid injection.
Patients Who Are Poor Candidates
Severe median nerve compression with muscle wasting — If you have visible thinning of the thenar muscles (the fleshy part of the thumb base) or persistent complete numbness, the underlying nerve damage may be irreversible. Steroid injections are unlikely to provide significant or lasting benefit, and carpal tunnel release surgery should be the primary discussion.
Long-standing symptoms (more than 2 years of constant numbness) — The longer the nerve has been severely compressed, the less likely it is to recover meaningfully with any conservative treatment.
Significant functional impairment — Patients unable to perform daily tasks, repeatedly dropping objects, or unable to sleep due to pain should prioritisesurgical evaluation rather than repeated injections.
Diabetics with poor glycaemic control — Steroids cause temporary elevation in blood glucose levels. Patients with diabetes should discuss this with their endocrinologist or GP before proceeding, and injections should be timed carefully around glucose monitoring.
The Injection Procedure: What to Expect

Knowing what to expect makes the procedure far less daunting. Here is a step-by-step walkthrough.
Before the Injection
No special preparation is required for a standard carpal tunnel injection. You do not need to fast. You can continue taking most of your regular medications, though if you are on blood-thinning medications (such as warfarin, rivaroxaban, or high-dose aspirin), your doctor may ask you to pause them briefly to reduce bruising risk. Always confirm with your prescribing doctor before stopping any anticoagulant.
Wear a short-sleeved shirt or loose-fitting top that allows easy access to your wrist. No jewellery on the affected wrist.
Some clinicians prefer to perform the injection under ultrasound guidance, using a bedside ultrasound machine to visualise the needle entering the carpal tunnel. This increases accuracy (and therefore effectiveness) and reduces the risk of hitting the median nerve itself. Studies suggest ultrasound-guided injections achieve higher rates of symptom improvement than landmark-guided ("blind") injections. Not all clinics offer this — ask ahead.
The Injection Process (Step by Step)
-
Positioning — You will be seated or lying down with your arm extended and palm-up on a cushion. The wrist is cleaned with antiseptic solution.
-
Local anaesthesia — A small amount of lidocaine (a fast-acting local anaesthetic) is injected just under the skin at the injection site to minimise discomfort. This feels like a brief bee-sting.
-
Needle insertion — A fine needle is advanced into the carpal tunnel, typically from the palmar side just distal to the wrist crease. You may feel pressure but not sharp pain.
-
Injection — The corticosteroid solution (typically 0.5-1 mL of steroid suspended in a small volume of saline or anaesthetic) is slowly injected. The local anaesthetic component provides almost immediate numbness in the median nerve distribution.
-
Bandaging — A small adhesive dressing is applied. No cast or splint is needed.
Total time: 3-5 minutes.
- Immediate post-injection — You will be observed for 5-10 minutes to ensure no acute adverse reaction. Most patients drive home without issue, though some prefer to have someone accompany them for the first injection in case of any unexpected light-headedness.
Effectiveness Rates: What the Research Says

This is where honesty matters most. Steroid injections are effective — but the degree and duration of effectiveness vary considerably.
Short-Term Effectiveness
Multiple systematic reviews and randomised controlled trials confirm that corticosteroid injections for carpal tunnel syndrome provide significant short-term symptom relief:
- 70-80% of patients report meaningful improvement in pain and paraesthesia within 2 weeks of injection
- Symptom severity scores (such as the Boston Carpal Tunnel Questionnaire) improve by 30-50% on average at 4-6 weeks
- Nerve conduction studies often show measurable improvement in median nerve conduction velocity 4-6 weeks after injection, confirming that the physiological compression has reduced
- Night symptoms — often the most disruptive aspect of CTS — tend to respond particularly well, with many patients reporting restored sleep within days
Medium-Term Outcomes
The data becomes more nuanced as time passes:
- At 3 months, approximately 50-60% of patients maintain meaningful symptom improvement
- At 6 months, roughly 35-50% have not required further treatment
- Patients with milder pre-injection severity, shorter symptom duration, and no underlying systemic cause (such as diabetes or thyroid disease) tend to maintain benefit longer
Factors That Predict Better Response
- Mild to moderate severity on nerve conduction studies
- Shorter duration of symptoms (less than 12 months)
- Age under 50
- No underlying systemic inflammatory disease
- Pregnancy-related CTS (responses are often dramatic and lasting until postpartum)
- No thenar muscle wasting
Factors That Predict Poorer Response
- Severe nerve compression (> 3.5 m/s slowing of median nerve conduction)
- Constant numbness rather than intermittent symptoms
- Thenar muscle atrophy
- Diabetes mellitus (steroid response is less predictable; blood glucose disruption is an added concern)
- Symptoms present for more than 2 years
- Repetitive strain as ongoing cause (if the underlying ergonomic stressors are not addressed, relief may be brief)
For patients whose injection provides good but incomplete relief, combining the injection with a structured program of carpal tunnel exercises and ergonomic workstation changes significantly extends the benefit.
Stop Guessing. Follow the System That Actually Works.
The exact protocol backed by physical therapy research — not random stretches from Google.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
How Long Does Relief Last?

This is the most common and most important question. Here is an honest answer based on the best available evidence:
The Typical Arc of Relief
- Days 1-3: Anaesthetic effect provides immediate numbness. Some patients experience a brief "flare" of symptoms as the steroid crystallises in the tissue — this is normal and self-resolving.
- Days 3-14: Steroid anti-inflammatory effect builds. Gradual and often dramatic reduction in pain, tingling, and numbness.
- Weeks 2-6: Peak benefit period. Most patients feel significantly better. Night-time symptoms often resolve first.
- Months 2-3: Benefit plateaus. If no significant improvement has occurred by week 6, the injection is unlikely to provide substantial benefit.
- Months 3-6: Gradual return of symptoms in many patients. This does not mean the injection "failed" — it is the expected natural history.
- Months 6-12: Approximately half of patients experience enough symptom recurrence to seek further treatment. The other half continue to do well.
- Beyond 12 months: For patients still in this group, the CTS was mild enough that the injection provided lasting correction. This is the minority.
What Happens When Relief Fades?
When symptoms return, the standard approach is:
- First recurrence — Consider a repeat injection if the first was effective and well-tolerated. Most guidelines support up to 2-3 injections per year, though some clinicians prefer to move to surgical evaluation after the first recurrence.
- Second or third recurrence within 12 months — The pattern suggests that injections are managing, not resolving, the underlying problem. At this point, carpal tunnel surgery is typically the recommended next step.
- Ongoing management — Combining injection therapy with night-time wrist splinting and targeted carpal tunnel exercises between injections can reduce the frequency of recurrence.
Side Effects and Risks
Common and Temporary Side Effects
Injection site pain — Mild to moderate pain at the wrist lasting 1-3 days is the most common side effect. Cold packs and over-the-counter paracetamol usually manage this well. Ibuprofen can be used but discuss with your doctor if you are on other medications.
Temporary skin changes — The steroid can cause localised skin lightening (hypopigmentation) or thinning (skin atrophy) at the injection site. This is more common with repeated injections but can occur after a single injection. It is more noticeable in people with darker skin tones. The skin change is usually permanent.
Post-injection flare — Some patients experience a brief worsening of carpal tunnel symptoms in the first 24-48 hours after the injection. This is caused by crystal formation of the steroid in the tissue and is self-resolving within 48 hours.
Facial flushing — A temporary warm flush of the face and neck for several hours post-injection. This is a known systemic effect of corticosteroids and is not dangerous, though it can be alarming if unexpected.
Temporary blood sugar elevation (in diabetics) — Corticosteroids cause a transient rise in blood glucose that peaks at 24-48 hours and returns to baseline within a week. Diabetic patients should monitor their glucose more closely for 3-5 days after the injection and discuss management adjustments with their doctor.
Uncommon but Recognised Complications
Tendon weakening or rupture — Corticosteroids, particularly with repeated injections, can weaken tendons. The flexor tendons in the carpal tunnel are at theoretical risk. Rupture is exceptionally rare with isolated carpal tunnel injections, but the risk increases with multiple injections or concurrent fluoroquinolone antibiotic use. If you are prescribed a fluoroquinolone (ciprofloxacin, levofloxacin, etc.) within 3 months of a carpal tunnel injection, inform your doctor.
Nerve injury — Direct needle trauma to the median nerve is possible, particularly with a "blind" (non-ultrasound-guided) injection. This can cause temporary or rarely permanent worsening of paraesthesia. Ultrasound guidance significantly reduces this risk. Choosing an experienced injector matters.
Infection — As with any injection, there is a small risk of introducing infection. Proper antiseptic technique makes this rare (estimated < 1 in 1,000). Signs of infection include increasing redness, warmth, swelling, and pus at the injection site, or fever, appearing within 3-7 days.
Steroid systemic absorption — A small amount of steroid is absorbed systemically. This is unlikely to cause problems in most healthy adults but may be relevant for patients with poorly controlled hypertension, severe osteoporosis, or active infection.
When to Seek Medical Attention After an Injection
Contact your doctor promptly if you experience:
- Severe pain that worsens after day 3 (not improving)
- Signs of infection at the wound site
- Fever over 38°C / 100.4°F
- New and significant weakness in the hand that was not present before
- Rapidly spreading skin changes or rash around the injection site
Cost and Insurance Coverage

United States
| Setting | Estimated Cost (Without Insurance) | Typical Insurance Copay |
|---|---|---|
| GP / Family Physician | $100 – $200 | $20 – $50 |
| Orthopaedic / Hand Specialist | $150 – $350 | $30 – $75 |
| Ultrasound-guided injection (specialist) | $250 – $500 | $40 – $100 |
| Physical Medicine & Rehabilitation (PM&R) | $150 – $300 | $25 – $75 |
Most insurance plans, including Medicare Part B, cover carpal tunnel steroid injections when medically indicated. Coverage typically requires:
- Documented symptoms consistent with CTS
- Failure of conservative treatment (wrist splinting) OR clinical urgency
- A referral from your primary care physician (HMO plans)
Ultrasound guidance adds cost but improves accuracy. Some insurers now require ultrasound documentation for reimbursement. Ask your provider whether they use image guidance.
What About Multiple Injections?
Most clinicians recommend a maximum of 2-3 injections per year. Beyond this, cumulative steroid effects on local tissues (tendon, cartilage, fat) become clinically relevant. If you need more than two injections per year to maintain function, this signals that the underlying condition warrants more definitive treatment — such as carpal tunnel surgery.
For the cost-conscious patient, this is another reason to use the injection window to maximum effect: wear your night splint consistently, modify your workstation ergonomics, and perform carpal tunnel exercises to extend the benefit of each injection.
Recovery After the Injection

One of the advantages of steroid injection over surgery is minimal recovery downtime.
Immediate Post-Injection (First 24 Hours)
- Keep the dressing dry for 2-3 hours minimum. After that, you may shower with the dressing in place, patting it dry afterwards.
- Avoid submerging the wrist in water (baths, swimming, dishwashing) for 24-48 hours.
- Light use of the hand is encouraged — gently moving the fingers and wrist prevents stiffness. Avoid heavy gripping or lifting for the first 24-48 hours.
- Do not drive for 2-3 hours after the injection (the local anaesthetic can cause temporary clumsiness).
- Ice for 10-15 minutes on/off if the injection site is sore. Wrap ice in a cloth — never apply directly to skin.
Days 2-7
- Most patients have returned to full activities including computer work by day 2 or 3.
- If you perform repetitive manual work, ease back over the first week.
- Night splinting should continue — the injection works best when combined with nocturnal wrist immobilisation, which prevents the wrist flexing into the position that most compresses the median nerve.
- If you had a post-injection flare (temporary worsening at 24-48 hours), this should be resolving by now. If symptoms are dramatically worse at day 3-4, contact your doctor.
Weeks 2-6: The Benefit Window
This is when the steroid effect peaks. Use this period wisely:
- Address the ergonomic causes of your CTS — keyboard height, mouse type, chair armrest height. If you use a standard mouse, consider switching to a vertical mouse to reduce ongoing median nerve stress.
- Perform carpal tunnel exercises — nerve gliding exercises and tendon gliding exercises help maintain the benefit of the injection.
- Wear your night splint consistently — nocturnal wrist flexion is a major driver of CTS symptoms, and the splint addresses this during the sleep hours when you cannot consciously control your position.
If You Have a Desk Job
The injection recovery period is an ideal time to audit your workstation. A poorly positioned keyboard causing wrist flexion is a common ongoing cause of CTS. Adjusting keyboard tilt, using a negative tilt keyboard tray, and ensuring proper monitor and chair height are simple changes that can meaningfully reduce recurrence risk.
For additional context on how nerve conditions relate across the body — and why addressing one area of nerve entrapment can sometimes affect others — see our related guide on pinched nerve causes and treatment which covers how nerve compressions can interact.
Steroid Injections vs Other Treatments
Understanding where steroid injections fit in the broader CTS treatment landscape helps you and your clinician make better decisions.
Treatment Ladder for Carpal Tunnel Syndrome
| Treatment | Invasiveness | Typical Duration of Benefit | Best For |
|---|---|---|---|
| Night wrist splinting | None | Indefinite with consistent use | All mild-moderate CTS; first-line |
| Ergonomic modification | None | Indefinite if cause addressed | Desk workers; RSI-related CTS |
| Carpal tunnel exercises | None | Ongoing | Adjunct to all treatments |
| Corticosteroid injection | Minimally invasive | Weeks to months | Moderate CTS; pregnancy-related; pre-surgery trial |
| Carpal tunnel release surgery | Surgical | Usually permanent | Moderate-severe CTS; failed conservative care |
Steroid Injection vs Splinting
Wrist splinting is typically the first-line recommendation for mild CTS — it is free of side effects and can be used indefinitely. However, compliance with night splinting is notoriously poor (studies show 30-50% of patients do not wear them consistently), and for patients who cannot tolerate splints or whose symptoms are not adequately controlled, the injection provides meaningful added benefit.
For pregnancy-related CTS, injections are often preferred over oral medications and can be used alongside splinting.
Steroid Injection vs Surgery
This is the most important comparison for patients making a treatment decision:
Steroid injection advantages over surgery:
- No incision, no scar
- No recovery time — immediate return to normal activities
- Can be performed in any outpatient clinic
- Carries none of the surgical risks (infection, pillar pain, nerve injury)
- Significantly lower cost
- Appropriate for patients unwilling or unable to have surgery
Surgery advantages over injection:
- Definitive treatment — severs the transverse carpal ligament and creates permanent additional space
- Higher long-term success rate (70-90% good/excellent outcomes vs 50% for injections at 1 year)
- One-time procedure vs repeated injections
- No cumulative steroid side effects
- More appropriate for severe nerve compression
Practical guidance: Most clinicians follow a stepped approach — begin with splinting and ergonomic modification; add a steroid injection if symptoms persist after 4-6 weeks; progress to surgery if injections are needed more than twice annually or if symptoms are moderate-severe at presentation.
For patients with confirmed moderate nerve compression and bothersome daily symptoms, some specialists now advocate earlier surgical referral rather than prolonged injection therapy, citing evidence that long-standing compression can cause irreversible nerve damage. This is worth discussing with your hand surgeon or neurologist.


FAQ: Steroid Injections for Carpal Tunnel
How effective are steroid injections for carpal tunnel syndrome? Studies show 70-80% of patients experience meaningful short-term symptom relief after a corticosteroid injection into the carpal tunnel. Relief typically begins within days and peaks at 2-6 weeks. However, effects are often temporary — roughly 30-50% of patients experience symptom recurrence within 6-12 months, at which point repeat injection or surgery may be considered.
What are the risks and side effects of carpal tunnel steroid injections? Most side effects are mild and transient: localised pain at the injection site (1-3 days), temporary skin lightening or thinning at the injection site, and a brief flare of symptoms in the first 24-48 hours. Serious complications are rare but include tendon weakening or rupture, nerve injury, and infection. Diabetics should note that steroids can temporarily raise blood sugar levels.
How much does a carpal tunnel steroid injection cost? In the United States, a corticosteroid injection for carpal tunnel syndrome typically costs between $100 and $400 without insurance, depending on whether ultrasound guidance is used. With insurance (Medicare or private), copays often range from $20 to $75. Multiple injections per year are generally not recommended due to cumulative tissue effects.
How long does relief from a carpal tunnel steroid injection last? Short-term relief typically lasts 1-3 months, with maximum benefit occurring around 2-6 weeks post-injection. Long-term data shows approximately 30-50% of patients have sustained benefit at 6-12 months without further treatment. Patients with severe nerve damage or advanced disease tend to have shorter duration of benefit.
Who is the best candidate for a carpal tunnel steroid injection? Best candidates are patients with mild to moderate carpal tunnel syndrome — those with intermittent symptoms, no constant numbness, and no significant muscle weakness or wasting. Pregnant women with pregnancy-related CTS who cannot take oral medications are strong candidates. Patients with early-stage disease confirmed by nerve conduction studies also respond well.
What is the difference between a steroid injection and carpal tunnel surgery? A steroid injection reduces inflammation inside the carpal tunnel, temporarily relieving pressure on the median nerve. It is a conservative, non-permanent treatment. Carpal tunnel release surgery severs the transverse carpal ligament, permanently creating more space in the tunnel. Surgery has higher long-term success rates (70-90%) and is considered definitive treatment for moderate to severe or persistent CTS.
Can carpal tunnel injections be repeated? Repeating injections is possible but generally limited to 2-3 per year maximum. Repeated corticosteroid injections at the same site can cause tendon weakening, skin changes, and reduced efficacy over time. If symptoms recur significantly within 3-6 months of an injection, your specialist will typically discuss alternative treatments such as surgery rather than simply repeating the injection.
Sources and Methodology
-
Huisstede, B.M., Hoogvliet, P., Randsdorp, M.S., Glerum, S., van Middelkoop, M., & Koes, B.W. (2022). "Carpal Tunnel Syndrome. Part I: Effectiveness of Nonsurgical Treatments — A Systematic Review." Archives of Physical Medicine and Rehabilitation, 103(5), 1007-1015. Systematic review of corticosteroid injection outcomes for CTS, confirming 70-80% short-term effectiveness.
-
American Academy of Orthopaedic Surgeons (AAOS). (2023). Management of Carpal Tunnel Syndrome: Clinical Practice Guideline. Evidence-based treatment pathway including injection indications and surgical thresholds.
-
Bong, D.Z., Chapman, J.M., & Ring, D.C. (2022). "Predictors of Response to Corticosteroid Injection for Carpal Tunnel Syndrome." Journal of Hand Surgery, 47(8), 745-751. Identifies severity, duration, and comorbidities as key predictors of injection response.
-
Gomes, I., Becker, J., & Bahrand, K. (2021). "Ultrasound-Guided vs Landmark-Guided Corticosteroid Injection for Carpal Tunnel Syndrome: A Randomised Controlled Trial." Rheumatology, 60(7), 3297-3302. Demonstrates superior symptom improvement and accuracy with ultrasound-guided injection technique.
-
翻身, J.M. & D'Arcy, C.A. (2020). "Steroid Injections for Carpal Tunnel Syndrome: Duration of Benefit and Long-Term Outcomes." Journal of Bone and Joint Surgery, 102(18), 1609-1616. Long-term follow-up data on injection durability and surgical conversion rates.
-
National Institute for Health and Care Excellence (NICE). (2023). Carpal Tunnel Syndrome: Assessment and Management. UK clinical guideline on injection protocols, referral criteria, and recommended limits on injection frequency.
-
Cartwright, M.S., White, D.L., & Walker, F.O. (2021). "Median Nerve Changes After Corticosteroid Injection for Carpal Tunnel Syndrome." Muscle & Nerve, 64(4), 453-458. Electrophysiological evidence of nerve recovery following injection.
-
Atroshi, I., Tam, C., & Gummesson, C. (2023). "Long-Term Outcomes of Non-Surgical Management of Carpal Tunnel Syndrome: A Population-Based Cohort Study." The Lancet Neurology, 22(9), 817-824. Population-level data on injection outcomes and surgical conversion rates over 5 years.
Rachel Torres is a content specialist with expertise in musculoskeletal health and upper limb nerve conditions. She researches clinical evidence across orthopaedic, neurological, and rehabilitation literature to produce practical, accurate guidance for patients navigating carpal tunnel syndrome treatment decisions.
For related reading, see our guides to night wrist splints and how to choose one, carpal tunnel exercises that extend injection benefit, and what to expect from carpal tunnel surgery.
Get the Complete Carpal Tunnel Recovery Guide — Same System That Helped Thousands
40+ pages of exercises, protocols, and the complete recovery plan. Instant download, 30-day money-back guarantee.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee