Guide
Tinnitus from Ear Infection: Causes, Treatment and When It Stops (2026)
By Dr. Karen L., Audiologist & ENT Specialist · Updated 2026-03-10
By Dr. Karen L., Audiologist & ENT Specialist | Last updated: March 2026
Ear infections are one of the most common — and most treatable — causes of tinnitus. When bacteria or viruses infect the outer, middle, or inner ear, the resulting inflammation, fluid buildup, and pressure changes can disrupt normal sound conduction and trigger ringing, buzzing, or humming in the affected ear. The good news: in most cases, tinnitus caused by an ear infection resolves within one to six weeks once the underlying infection is properly treated with antibiotics, antivirals, or supportive care.
This article contains affiliate links. See our affiliate disclosure for details.
Table of Contents
- How Ear Infections Cause Tinnitus
- Types of Ear Infections That Trigger Tinnitus
- Symptoms: What Ear Infection Tinnitus Sounds Like
- Treatment Options
- Ear Health and Tinnitus Relief Products
- Recovery Timeline: When Does the Ringing Stop?
- When to See a Doctor
- Prevention: How to Protect Your Ears
- Frequently Asked Questions
- About the Author
- Sources
How Ear Infections Cause Tinnitus
To understand why ear infections trigger tinnitus, it helps to know how your ear processes sound under normal conditions.
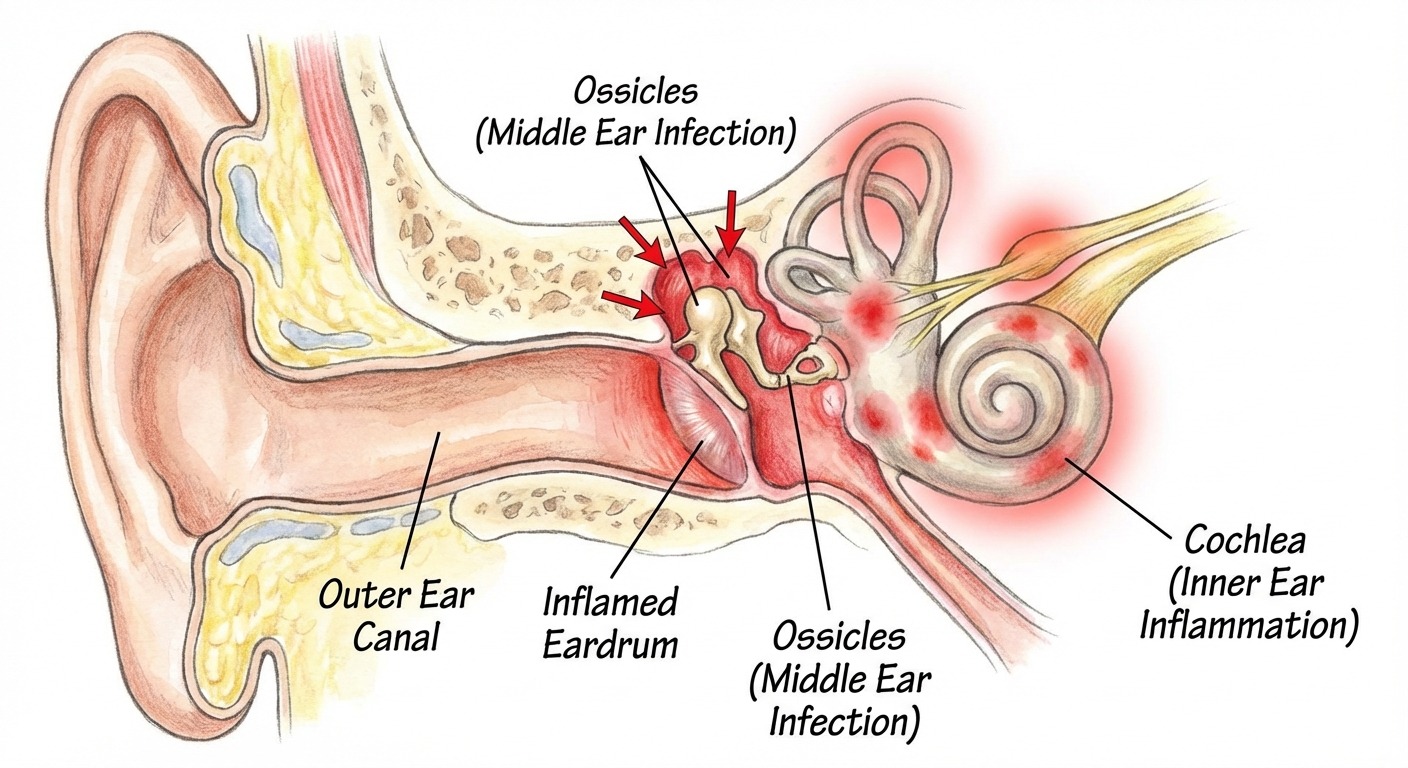
Sound waves travel through the ear canal, vibrate the eardrum (tympanic membrane), and pass through three tiny bones in the middle ear — the malleus, incus, and stapes. These bones amplify the vibrations and transmit them to the fluid-filled cochlea in the inner ear. Inside the cochlea, thousands of microscopic hair cells convert those vibrations into electrical signals that travel along the auditory nerve to the brain, where they are interpreted as sound.
An ear infection disrupts this chain at one or more points. Here is what happens:

- Inflammation — Swollen tissues in the ear canal or middle ear physically alter how sound vibrations travel, creating abnormal signals that the brain may interpret as ringing or buzzing.
- Fluid buildup — Infections, especially middle ear infections, cause pus or serous fluid to accumulate behind the eardrum. This fluid dampens eardrum vibrations and changes the impedance (resistance) of the middle ear system. The brain, receiving weaker or distorted signals, may generate phantom sound to compensate.
- Pressure changes — Blocked eustachian tubes prevent the middle ear from equalizing pressure with the outside environment. This pressure differential stretches the eardrum and alters ossicle movement, producing a sensation of fullness and often tinnitus.
- Direct nerve irritation — Inner ear infections (labyrinthitis, vestibular neuritis) inflame the cochlear nerve or damage the hair cells directly, sending aberrant electrical signals to the auditory cortex.
- Conductive hearing loss — When infection reduces the ear's ability to conduct sound efficiently, the brain turns up its internal "gain" to compensate for the reduced input — and this amplification can produce or worsen tinnitus.
According to a 2023 systematic review published in the International Journal of Audiology, approximately 30 to 40 percent of patients with acute otitis media report tinnitus as a concurrent symptom, and the prevalence rises to over 60 percent in cases of labyrinthitis.
Understanding which part of the ear is affected helps predict how severe the tinnitus may be and how quickly it will resolve.
Types of Ear Infections That Trigger Tinnitus
Not all ear infections carry the same risk for tinnitus. The location, severity, and duration of the infection all influence whether ringing develops and how long it lasts.
Outer Ear Infection (Otitis Externa / Swimmer's Ear)
Otitis externa is an infection of the ear canal — the tube that runs from the outer ear to the eardrum. It is commonly called "swimmer's ear" because moisture trapped in the ear canal creates an ideal environment for bacterial growth.
How it causes tinnitus: Swelling of the ear canal narrows the passage, altering the way sound reaches the eardrum. In severe cases, the canal can swell shut entirely, creating significant conductive hearing loss and triggering tinnitus. Debris and discharge from the infection can also press against the eardrum.
Tinnitus characteristics: Typically low-pitched, intermittent, and mild. Most patients describe it as a dull hum or muffled sensation rather than a sharp ring.
Prognosis: Tinnitus from otitis externa usually resolves within one to two weeks once the infection is treated with antibiotic ear drops. This is the least likely type of ear infection to cause lasting tinnitus.
Middle Ear Infection (Otitis Media)
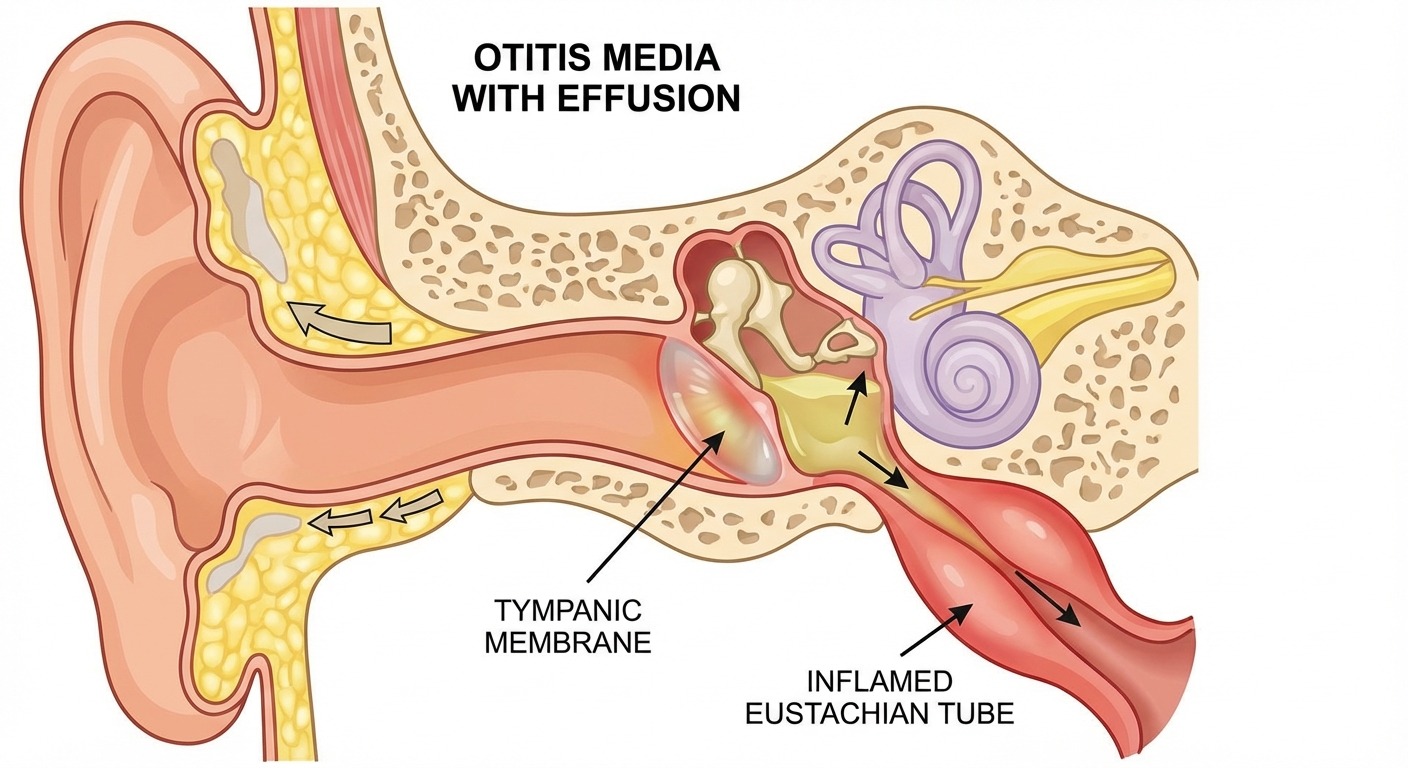
Otitis media is the most common type of ear infection, particularly in children. It occurs when bacteria or viruses infect the space behind the eardrum, usually following an upper respiratory infection or allergies that block the eustachian tube.
How it causes tinnitus: Fluid accumulation behind the eardrum is the primary mechanism. This effusion dampens the eardrum's ability to vibrate freely and restricts the movement of the ossicles. The resulting conductive hearing loss triggers the brain's compensatory gain mechanism, producing tinnitus. Additionally, pressure from the trapped fluid can directly stimulate the nerve endings in the middle ear.
Tinnitus characteristics: Often described as a low-pitched roaring, rumbling, or pulsating sound. Some patients report hearing their own heartbeat (pulsatile tinnitus) due to increased blood flow to the inflamed area. The tinnitus is usually unilateral — affecting only the infected ear.
Prognosis: With proper antibiotic treatment, tinnitus from otitis media typically resolves within two to four weeks. However, if fluid persists in the middle ear after the active infection clears (a condition called serous otitis media or "glue ear"), tinnitus may continue for six to twelve weeks until the fluid fully drains.
Chronic otitis media — defined as infection lasting more than three months or recurring three or more times in six months — carries a higher risk of persistent tinnitus and may require surgical intervention such as tympanostomy tube placement.
Inner Ear Infection (Labyrinthitis and Vestibular Neuritis)
Inner ear infections are less common but significantly more serious in terms of tinnitus risk. Labyrinthitis involves inflammation of the labyrinth — the structure containing both the cochlea (hearing) and the vestibular system (balance). Vestibular neuritis affects only the vestibular nerve.
How it causes tinnitus: Labyrinthitis directly inflames the cochlea and the cochlear nerve, damaging the delicate hair cells responsible for sound detection. Unlike outer and middle ear infections that disrupt sound conduction, inner ear infections disrupt the sensorineural pathway — the electrical signaling system itself. This type of damage is more likely to produce persistent tinnitus.
Tinnitus characteristics: Higher-pitched ringing, hissing, or whistling. Often accompanied by vertigo (a spinning sensation), nausea, and sensorineural hearing loss. The tinnitus may be constant rather than intermittent.
Prognosis: Tinnitus from labyrinthitis can take four to twelve weeks to resolve, and in some cases may become chronic. According to the Vestibular Disorders Association, approximately 50 percent of labyrinthitis patients experience some degree of residual tinnitus after the acute phase. Early treatment with corticosteroids and antivirals (if the cause is viral) improves outcomes significantly.
Comparison Table: Ear Infection Types and Tinnitus
| Feature | Outer Ear (Otitis Externa) | Middle Ear (Otitis Media) | Inner Ear (Labyrinthitis) |
|---|---|---|---|
| Location | Ear canal | Behind eardrum | Cochlea / vestibular system |
| Common cause | Bacteria, moisture | Bacteria, viruses, allergies | Viral, bacterial |
| Tinnitus type | Low hum, mild | Roaring, pulsating | High-pitched ring, hiss |
| Hearing loss | Conductive (mild) | Conductive (moderate) | Sensorineural |
| Vertigo | Rare | Uncommon | Common |
| Tinnitus duration | 1–2 weeks | 2–4 weeks | 4–12+ weeks |
| Risk of permanent tinnitus | Very low | Low–moderate | Moderate–high |
Symptoms: What Ear Infection Tinnitus Sounds Like
Tinnitus caused by ear infections has some distinct characteristics that differentiate it from other types:
- Onset timing — The ringing typically begins during or shortly after the infection develops, rather than gradually over months or years.
- Sound quality — Most patients describe a low-pitched buzzing, humming, or roaring sound. Inner ear infections may produce a higher-pitched hiss or ring.
- Unilateral presentation — Ear infection tinnitus usually affects only the infected ear, making it easier to identify the cause.
- Pulsatile component — Middle ear infections commonly produce pulsatile tinnitus (hearing your heartbeat) due to increased blood flow and fluid pressure.
- Associated symptoms — Unlike age-related or noise-induced tinnitus, ear infection tinnitus is almost always accompanied by ear pain, pressure, hearing reduction, and sometimes fever or discharge.
- Fluctuation — The intensity often changes with head position or when swallowing, yawning, or blowing the nose — activities that affect eustachian tube function and middle ear pressure.
If you are experiencing tinnitus alongside any of these symptoms, an ear infection is a strong possibility and you should see a healthcare provider for examination. The sooner the infection is treated, the sooner the tinnitus will resolve.
For a deeper understanding of all the factors that can trigger ringing in the ears, read our complete guide on what causes tinnitus.
Treatment Options
Treatment for ear infection tinnitus focuses on resolving the underlying infection. Once the infection clears, tinnitus typically follows. Here are the evidence-based treatment approaches organized by infection type.
Treating Outer Ear Infections
- Antibiotic ear drops — Ciprofloxacin or ofloxacin drops are the first-line treatment. Drops are applied directly to the ear canal 2–3 times daily for 7–10 days.
- Ear canal cleaning — Your doctor may gently suction or wick out debris and discharge to allow the drops to reach the infected tissue.
- Pain management — Over-the-counter ibuprofen or acetaminophen for discomfort. Warm compresses applied externally can also help.
- Keep ears dry — Avoid swimming, use earplugs during bathing, and do not insert cotton swabs or any objects into the ear.
Treating Middle Ear Infections

- Oral antibiotics — Amoxicillin is the standard first-line antibiotic for bacterial otitis media. A typical course is 7–10 days. According to the American Academy of Otolaryngology, antibiotic therapy resolves middle ear infections in approximately 80 percent of cases.
- Decongestants and nasal corticosteroids — These help open the eustachian tube, allowing trapped fluid to drain from the middle ear. Pseudoephedrine and fluticasone nasal spray are common options.
- Watchful waiting — For mild cases in adults, some doctors recommend a 48–72 hour observation period before prescribing antibiotics, as many middle ear infections resolve on their own. However, if tinnitus is present, most specialists recommend treating promptly to minimize symptom duration.
- Myringotomy and tubes — For chronic or recurrent middle ear infections with persistent fluid, a small incision in the eardrum (myringotomy) allows fluid drainage. Tiny ventilation tubes may be placed to keep the middle ear aerated. This procedure is performed under local anesthesia and provides rapid relief of both hearing loss and tinnitus.
Treating Inner Ear Infections
- Corticosteroids — Oral prednisone or intratympanic steroid injections reduce cochlear inflammation and may prevent permanent hair cell damage. Treatment is most effective when started within the first 72 hours of symptom onset.
- Antiviral medications — If viral labyrinthitis is suspected (often following a respiratory illness), antivirals such as valacyclovir may be prescribed alongside steroids.
- Vestibular suppressants — Medications like meclizine or diazepam help manage vertigo and nausea during the acute phase.
- Vestibular rehabilitation therapy — Once the acute phase resolves, physical therapy exercises help the brain compensate for any lasting balance deficits.
Managing Tinnitus During Recovery
While waiting for the infection to clear, these strategies can help manage the tinnitus itself:
- Sound therapy — Background sound from a white noise machine, fan, or sound therapy app can mask the tinnitus and reduce its perceived intensity. This is especially helpful at bedtime when tinnitus is most noticeable.
- Relaxation techniques — Stress and anxiety amplify tinnitus perception. Deep breathing, progressive muscle relaxation, and guided meditation can lower your stress response. For more on this connection, see our article on tinnitus and anxiety.
- Sleep hygiene — Tinnitus often worsens at night. Using a sound machine and maintaining consistent sleep schedules can break the tinnitus-insomnia cycle. If tinnitus and sleep disruption are significantly impacting your rest, dedicated sleep-focused sound machines may help.
- Avoid irritants — Reduce caffeine, alcohol, and sodium intake during recovery, as these can worsen tinnitus. Our guide on tinnitus remedies that actually work covers additional evidence-based management strategies.
Ear Health and Tinnitus Relief Products
The following products can support ear infection recovery and help manage tinnitus symptoms. Always consult your doctor before using any ear-related product during an active infection.

LectroFan White Noise Machine
20 unique sound options including white noise, fan sounds, and ocean waves. Ideal for masking tinnitus at night during ear infection recovery.
Why we recommend it: Consistent, non-looping sounds provide reliable tinnitus masking without sudden volume changes.
Check Price on Amazon
Mack's Pillow Soft Silicone Earplugs
Moldable silicone earplugs that seal over the ear canal opening without insertion. Keeps water out during showers and bathing.
Why we recommend it: Prevents moisture from entering the ear canal — critical during and after ear infection treatment.
Check Price on Amazon
Sound Oasis Tinnitus Sound Therapy System
Clinically designed sound therapy with 12 tinnitus-specific programs developed with audiologists. Portable bedside design.
Why we recommend it: Purpose-built for tinnitus relief with frequencies optimized to match common tinnitus pitches.
Check Price on Amazon
Debrox Earwax Removal Drops
Carbamide peroxide drops that gently soften and remove excess earwax. Use only after your infection has fully cleared.
Why we recommend it: Post-infection earwax buildup can prolong tinnitus. Safe at-home removal supports hearing recovery.
Check Price on Amazon
TheraPearl Hot/Cold Ear Pain Relief
Reusable gel pack shaped to fit around the ear. Use warm for pain relief or cold for inflammation reduction during acute infection.
Why we recommend it: Contoured design provides targeted thermal therapy directly to the affected ear area.
Check Price on AmazonFor additional sound therapy options, see our complete review of the best sound machines for tinnitus.
Recovery Timeline: When Does the Ringing Stop?
One of the most common questions patients ask is "when will the ringing stop?" The answer depends on the type and severity of infection, but here is what the research shows.
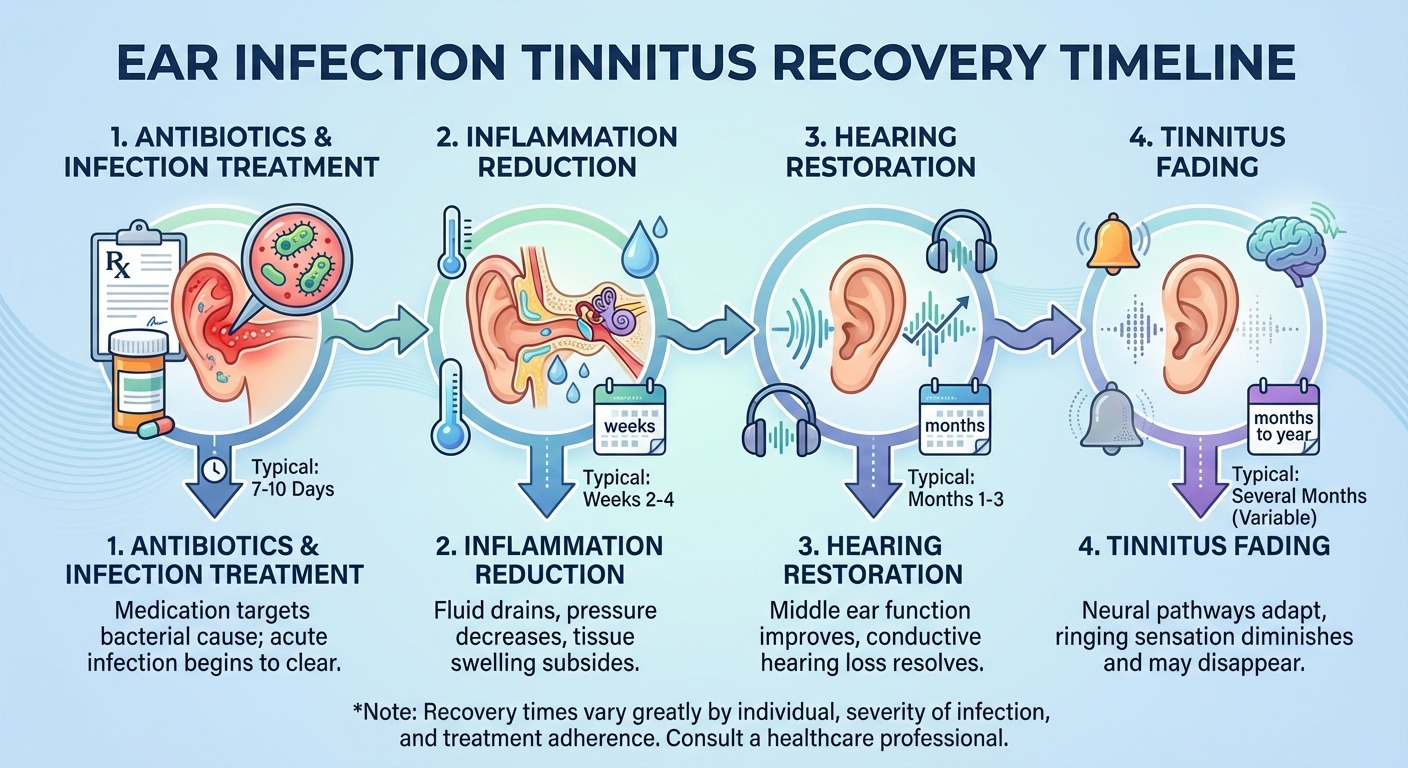
Phase 1: Active Infection (Days 1–10)
During the active infection, tinnitus is usually at its worst. Inflammation and fluid are at peak levels, and the ear's sound-conducting mechanisms are most disrupted. Antibiotics or antivirals begin working within 48–72 hours, and most patients notice a gradual reduction in ear pain and pressure during this phase.
What to expect: Tinnitus may actually seem louder in the first 2–3 days of treatment as inflammation peaks before subsiding. This is normal and does not indicate treatment failure.
Phase 2: Infection Clearing (Days 10–21)
The active infection resolves, but residual inflammation and fluid may persist. Hearing gradually improves as the eardrum regains normal mobility. Tinnitus typically shifts from constant to intermittent during this phase.
What to expect: You may notice the tinnitus comes and goes, particularly worsening at night or during quiet moments. This fluctuation is a positive sign of recovery.
Phase 3: Fluid Resolution (Weeks 3–6)
Remaining middle ear fluid gradually drains through the eustachian tube. As fluid clears, conductive hearing loss resolves and tinnitus continues to diminish.
What to expect: Brief episodes of ringing that last seconds to minutes, particularly when changing head position or after physical activity. These episodes should become progressively less frequent.
Phase 4: Full Resolution (Weeks 6–12)
For the majority of patients, all tinnitus symptoms have resolved by this point. The auditory system has returned to baseline function.
What to expect: Occasional, fleeting moments of very faint ringing that last only seconds. These transient episodes are common in the general population and are not a sign of persistent pathology.
When Recovery Takes Longer
Certain factors can delay tinnitus resolution:
- Pre-existing hearing loss — If you already had some degree of hearing loss before the infection, tinnitus may take longer to resolve or may unmask previously subclinical tinnitus.
- Repeated infections — Multiple ear infections cause cumulative damage to the middle ear structures.
- Delayed treatment — Infections treated more than a week after symptom onset have higher rates of complications, including prolonged tinnitus.
- Inner ear involvement — Labyrinthitis carries the highest risk of persistent tinnitus, with up to 50 percent of patients reporting some residual symptoms at 3 months (Vestibular Disorders Association).
- Ototoxic medications — Certain antibiotics used to treat severe infections (particularly aminoglycosides) can themselves cause tinnitus. Discuss this risk with your doctor.
If tinnitus persists beyond three months after your infection has cleared, consult an audiologist for a comprehensive hearing evaluation and tinnitus assessment.
When to See a Doctor

While mild ear infections sometimes resolve on their own, you should see a doctor promptly if you experience any of the following:
- Ear pain lasting more than 48 hours or severe ear pain at any point
- Fever above 101°F (38.3°C) accompanying ear symptoms
- Discharge or drainage from the ear, especially if bloody or foul-smelling
- Sudden or significant hearing loss in one or both ears
- Dizziness or vertigo — spinning sensation, difficulty with balance
- Tinnitus that worsens despite initial improvement in other symptoms
- Facial weakness or numbness on the side of the infected ear
- Symptoms in a child under 6 months, or any child with high fever and ear pain
- Recurrent infections — three or more episodes in six months
Seek Emergency Care If:
- Severe headache, stiff neck, or confusion (possible meningitis)
- High fever with ear drainage (possible mastoiditis — infection of the skull bone behind the ear)
- Sudden complete hearing loss
- Facial drooping on the affected side

Your doctor will use an otoscope to examine the ear canal and eardrum, and may order a tympanometry test to measure middle ear pressure and eardrum mobility. For suspected inner ear infections, an audiogram (hearing test) and possibly an MRI may be recommended to assess cochlear function and rule out other causes.
Prevention: How to Protect Your Ears
Preventing ear infections is the most effective way to avoid infection-related tinnitus. These evidence-based strategies significantly reduce your risk:
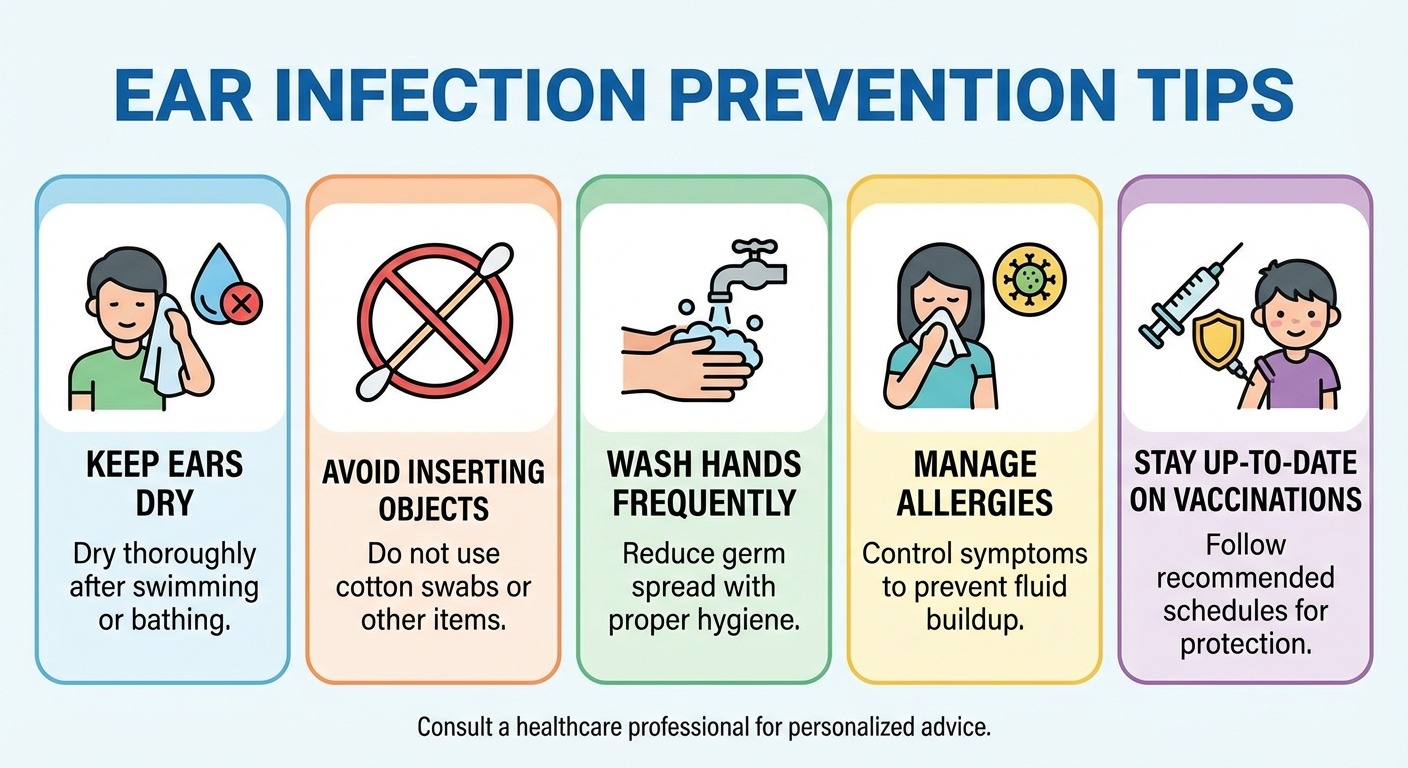
Keep Ears Dry
Moisture in the ear canal creates a breeding ground for bacteria. After swimming, showering, or bathing:
- Tilt your head to each side to drain water
- Gently dry the outer ear with a towel
- Use a hair dryer on the lowest, coolest setting held at arm's length
- Consider swimmer's earplugs if you swim regularly
Do Not Insert Objects Into the Ear Canal
Cotton swabs, bobby pins, and ear candles do more harm than good. They push wax deeper, can scratch the ear canal lining (creating entry points for bacteria), and risk perforating the eardrum. The ear canal is self-cleaning — wax naturally migrates outward.
Manage Allergies and Sinus Issues
Allergies cause eustachian tube swelling, which prevents middle ear drainage and increases infection risk. Treating allergies with antihistamines, nasal corticosteroids, or immunotherapy reduces the frequency of middle ear infections.
Practice Good Hygiene
Regular handwashing reduces transmission of the respiratory viruses and bacteria that frequently lead to secondary ear infections. This is especially important during cold and flu season.
Don't Smoke (and Avoid Secondhand Smoke)
According to the CDC, children exposed to secondhand smoke have significantly higher rates of ear infections. In adults, smoking damages the cilia in the eustachian tube, impairing drainage and increasing infection risk.
Stay Current on Vaccinations
The pneumococcal vaccine and annual flu vaccine reduce the incidence of bacterial and viral infections that commonly lead to ear infections.
Frequently Asked Questions
Can an ear infection cause permanent tinnitus?
Most ear infection tinnitus is temporary and resolves once the infection clears. However, severe or untreated infections — especially inner ear infections like labyrinthitis — can damage the cochlear hair cells and cause lasting tinnitus. Prompt treatment with antibiotics or antivirals significantly reduces the risk of permanent symptoms. According to the American Academy of Otolaryngology, fewer than 10 percent of acute ear infection cases result in tinnitus lasting longer than three months.
How long does tinnitus last after an ear infection?
For most people, tinnitus from an ear infection fades within one to six weeks after the infection resolves. Outer ear infections typically clear fastest (one to two weeks), middle ear infections take two to four weeks, and inner ear infections may take four to twelve weeks. If tinnitus persists beyond three months, consult an audiologist for a comprehensive evaluation.
What does tinnitus from an ear infection sound like?
Tinnitus caused by ear infections is most commonly described as a low-pitched humming, roaring, or buzzing sound. It may also present as a pulsing or throbbing sensation that matches your heartbeat, particularly with middle ear infections where fluid buildup creates pressure changes. Inner ear infections tend to produce higher-pitched ringing or hissing.
Should I see a doctor for ear infection tinnitus?
Yes, you should see a doctor if tinnitus is accompanied by ear pain, fever, drainage from the ear, sudden hearing loss, dizziness, or if the ringing persists for more than two weeks. Ear infections require proper diagnosis and often antibiotic treatment to prevent complications and speed tinnitus resolution.
Can ear drops help tinnitus from an ear infection?
Antibiotic ear drops can treat the underlying outer or middle ear infection, which in turn resolves the tinnitus. Over-the-counter drops should not be used if you suspect a perforated eardrum. Always get a proper diagnosis before using ear drops, as the wrong type can worsen the condition or cause pain.
Does fluid in the ear cause tinnitus?
Yes. Fluid accumulation in the middle ear — common during and after ear infections — alters sound conduction and creates pressure imbalances that the brain interprets as tinnitus. The ringing usually stops once the fluid drains naturally or with medical treatment. In persistent cases, tympanostomy tubes can provide immediate drainage and relief.

About the Author
Dr. Karen L. is a board-certified audiologist and ENT specialist with over 15 years of clinical experience in diagnosing and treating hearing disorders, tinnitus, and balance conditions. She completed her Doctor of Audiology (Au.D.) at the University of Pennsylvania and her clinical fellowship at Johns Hopkins Medicine. Dr. Karen has published research on infection-related hearing loss in the American Journal of Audiology and serves as a clinical reviewer for TinnitusGuides.com. Her approach emphasizes evidence-based treatment and empowering patients with the knowledge they need to manage their ear health effectively.
Sources
-
National Institute on Deafness and Other Communication Disorders (NIDCD) — Ear infections in children and adults: prevalence, diagnosis, and treatment guidelines. Source: nidcd.nih.gov/health/ear-infections-children
-
American Academy of Otolaryngology – Head and Neck Surgery — Clinical practice guideline: acute otitis externa (2014, updated 2021). Recommendations for diagnosis and management. Source: entnet.org
-
Mayo Clinic — Ear infection (middle ear) overview: symptoms, causes, diagnosis, and treatment. Source: mayoclinic.org/diseases-conditions/ear-infections
-
Vestibular Disorders Association (VeDA) — Labyrinthitis and vestibular neuritis: long-term outcomes, tinnitus prevalence, and rehabilitation protocols. Source: vestibular.org
-
International Journal of Audiology (2023) — Systematic review: tinnitus prevalence in acute and chronic otitis media. Findings indicate 30–40% concurrent tinnitus rate in acute cases and higher rates in chronic infections.
-
Centers for Disease Control and Prevention (CDC) — Antibiotic prescribing and use: ear infections. Guidance on appropriate antibiotic treatment and prevention strategies. Source: cdc.gov
-
British Medical Journal (BMJ) — Management of acute otitis media in adults: evidence-based review of treatment outcomes and tinnitus as a secondary symptom.
Medical Disclaimer
The information provided in this article is for educational and informational purposes only and is not a substitute for professional medical advice, diagnosis, or treatment. Always seek the advice of your physician, audiologist, or other qualified health provider with any questions you may have regarding an ear infection or tinnitus. Never disregard professional medical advice or delay in seeking it because of information you read on TinnitusGuides. If you experience severe ear pain, sudden hearing loss, high fever, or dizziness, contact your healthcare provider immediately. Individual results may vary.
Looking for more tinnitus relief strategies? Read our guide to the best sound machines for tinnitus or learn about tinnitus treatment at home.