Guide
Carpal Tunnel Brace vs. Surgery: Which Is Right for You? (2026)
By Rachel, Ergonomic Health Specialist · Updated 2026-04-21
If you have been diagnosed with carpal tunnel syndrome, you have likely been told two things: try a wrist brace first, and if that does not work, consider surgery. But the decision is rarely that straightforward. This guide breaks down everything you need to know to make an informed choice.
The Complete Carpal Tunnel Recovery System — Everything in One Guide
Exercises, stretches, ergonomic setups, brace recommendations, and a step-by-step daily program. 40+ pages, instant download.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
Table of Contents
- Understanding Carpal Tunnel Syndrome
- When a Wrist Brace Is the Right First Step
- When Surgery Becomes Necessary
- Comparing Recovery Times
- Success Rates and Long-Term Outcomes
- Cost Comparison: Brace vs. Surgery
- Risks and Complications
- How to Decide: A Decision Framework
- Frequently Asked Questions
- Sources & Methodology
Understanding Carpal Tunnel Syndrome
Carpal tunnel syndrome occurs when the median nerve, which runs from your forearm into your hand through a narrow tunnel of bone and ligament in your wrist, becomes compressed. This compression causes the numbness, tingling, weakness, and aching pain that characterizes the condition.
The carpal tunnel is already a tight space. When swelling of the surrounding tendons or tissues narrows it further, the median nerve gets squeezed. Repetitive hand movements, pregnancy, certain medical conditions like diabetes and rheumatoid arthritis, and even your anatomy can all contribute to this compression.
According to the American Academy of Orthopaedic Surgeons (AAOS), carpal tunnel syndrome affects approximately 4–10 million Americans, making it one of the most common nerve compression disorders. Women are three times more likely to develop it than men, and the condition most frequently appears in people aged 30–60.

The symptoms typically develop gradually. You may notice tingling in your thumb, index, and middle fingers, especially at night. As the condition worsens, you might experience weakness that makes it difficult to grip objects or perform fine motor tasks like buttoning your shirt. Without appropriate treatment, permanent nerve damage and muscle atrophy in the palm can result.
Understanding what is actually happening inside your wrist is the foundation for making the right treatment decision. A brace and surgery address the problem in fundamentally different ways, and the choice depends on how severe your compression is and how your body responds to conservative care.
When a Wrist Brace Is the Right First Step
A wrist brace, also called a wrist splint, is almost always the first-line treatment for carpal tunnel syndrome. The logic is straightforward: keeping your wrist in a neutral position reduces pressure inside the carpal tunnel, which allows the median nerve to breathe and recover.
The neutral position is critical. When your wrist is bent backward (extension) or sharply forward (flexion), the pressure inside the carpal tunnel increases dramatically. A well-designed wrist brace holds your wrist in roughly 0–15 degrees of extension, which is the position where tunnel pressure is at its lowest. This is why most doctors recommend wearing a brace specifically at night, since most people sleep with their wrists curled under a pillow in a flexed position.
There are two main types of wrist braces for carpal tunnel syndrome. A resting brace is designed to be worn during sleep and quiet times; it has a rigid outer shell and keeps your wrist fully immobilized. A working brace is more flexible, allowing some hand movement while still preventing the most damaging wrist positions. For daytime use during typing or manual work, a lighter, more flexible brace often works better than a heavy resting splint.

The research consistently supports bracing as an effective first-line treatment. A systematic review published in the Journal of Orthopaedic & Sports Physical Therapy found that wrist splinting produced significant symptom improvement in mild to moderate carpal tunnel syndrome, particularly when used consistently for at least three weeks. The key word is consistently. Wearing a brace sporadically, only when you remember, will not give the nerve time to recover.
Most people start to notice improvement within 2–4 weeks of consistent brace use. If you see no meaningful improvement after 6–8 weeks of full-time (including sleep) bracing, it is worth returning to your doctor to discuss whether more advanced interventions are needed. The absence of any response to conservative treatment is one of the clearest indicators that surgery may be necessary.
Braces are widely available over the counter at pharmacies and online retailers, with prices ranging from $15–$60. A doctor can also prescribe a custom-fitted orthosis if needed, though studies have not shown clear superiority of custom braces over well-designed OTC options for most cases.
When Surgery Becomes Necessary
Carpal tunnel release surgery, known medically as carpal tunnel decompression, becomes the recommended treatment when conservative measures fail to provide adequate relief, or when there is evidence of significant nerve damage that risks becoming permanent.
The most common indicator that it is time to consider surgery is failure of a structured conservative treatment program. This typically means 3–6 months of consistent bracing, activity modification, and possibly physical therapy without meaningful improvement. Your doctor may order electrodiagnostic testing, specifically nerve conduction studies and electromyography (EMG), to quantify how severely the median nerve is being compressed and whether the myelin sheath that insulates the nerve has been damaged.

Surgery is also recommended when certain red flags are present. These include constant numbness or tingling even with a brace, visible muscle wasting in the thenar eminence (the meaty part of your palm near the thumb), significant weakness in thumb opposition or grip strength, and sleep disruption severe enough that bracing at night does not help.
There are two primary surgical techniques. Open carpal tunnel release involves a single 2–3 inch incision in the palm, through which the surgeon cuts the transverse carpal ligament to relieve pressure on the nerve. Endoscopic carpal tunnel release uses one or two small incisions and a tiny camera to guide the blade, allowing the same ligament to be cut with less tissue disruption. The endoscopic technique generally results in less immediate post-operative pain and faster return to normal activities, though both approaches achieve comparable long-term outcomes.
The AAOS Clinical Practice Guidelines give a strong recommendation for surgical decompression in patients with confirmed median nerve compression and persistent symptoms that interfere with normal activities, even after conservative treatment has been attempted. Surgery is not a last resort in the sense that you should be afraid of it; when indicated, it is a highly effective solution that addresses the root mechanical cause of the problem.
Comparing Recovery Times
The recovery experience after treatment for carpal tunnel syndrome differs dramatically between bracing alone and surgery. Understanding what you are signing up for is an important part of the decision.
With bracing alone, there is no recovery period. You simply start wearing the brace and continue your normal activities, with modifications to avoid aggravating movements. Some people experience immediate relief from nighttime bracing, since that is when the wrist is most likely to be in a damaging position during sleep. Others need the full 4–6 weeks of consistent wear before noticing significant change.
The limitation of conservative treatment is that it manages the condition rather than resolving the underlying mechanical compression. If you stop wearing the brace and return to the same aggravating activities without ergonomic improvements, symptoms typically return. Bracing is therefore often a long-term management strategy rather than a cure.
After carpal tunnel surgery, recovery unfolds in stages. In the first 1–2 weeks, you will be in a bulky dressing and instructed to keep your hand elevated to control swelling. Most people can resume light activities like using a keyboard or phone within a few days to a week, though heavy gripping and lifting are restricted.
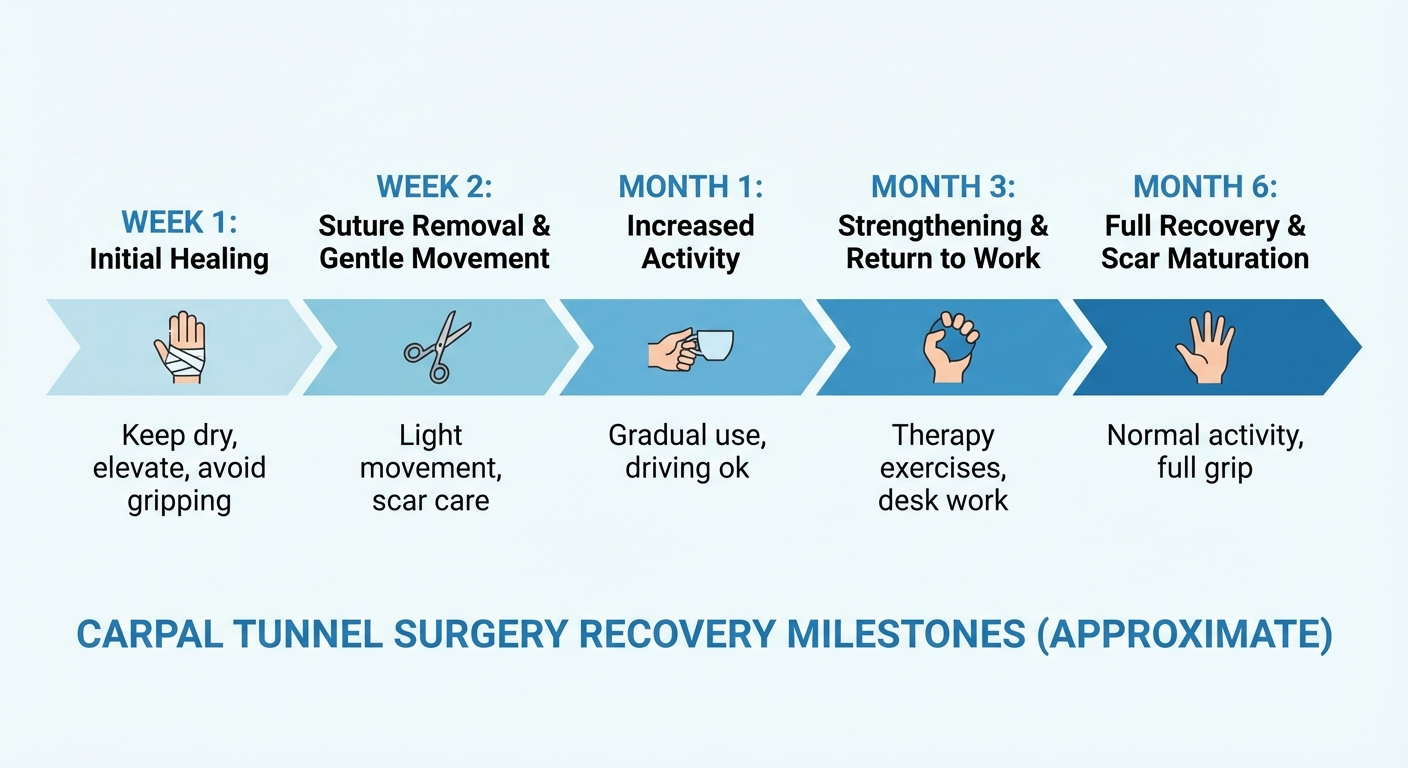
Between weeks 2 and 6, you transition from the surgical dressing to a lighter removable splint. You will begin working with a physical therapist to restore range of motion and gradually strengthen the hand. The pillar pain, which is the deep tenderness at the base of the palm where the ligament was cut, typically peaks during this phase and gradually subsides.
By weeks 6–12, most people have returned to full activities, including heavy lifting. Some residual pillar pain or stiffness may persist for several more months, particularly after open surgery. Endoscopic surgery tends to produce less pillar pain and faster resolution of post-operative discomfort.
Nerve recovery, however, moves at its own pace. The median nerve can take 6–12 months to fully regenerate after the compression is relieved. During this time, you may notice gradual improvement in strength, sensation, and fine motor coordination. Numbness that has been present for years may take months to fully resolve even after successful surgery, particularly if the nerve was severely compressed.
Stop Guessing. Follow the System That Actually Works.
The exact protocol backed by physical therapy research — not random stretches from Google.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee
Success Rates and Long-Term Outcomes
Both treatment approaches have strong track records, but they differ in predictability and what you can reasonably expect long-term.
Wrist braces, when used consistently in appropriate cases, produce meaningful symptom relief in approximately 70–80% of people with mild to moderate carpal tunnel syndrome. The limitation is that the effectiveness depends heavily on compliance. The moment you stop wearing the brace during aggravating activities or sleep, the benefit often reverses. Bracing is most effective as a long-term strategy when combined with ergonomic modifications that address the root causes of overwork in the wrist.
Carpal tunnel surgery has a higher and more reliable success rate. According to a large meta-analysis published in the Journal of Hand Surgery, carpal tunnel release achieves excellent or good outcomes in approximately 90% of cases. Symptom relief is typically sustained long-term, with recurrence rates of only 5–10% over a patient's lifetime.

The reason surgery tends to be more definitive is that it addresses the structural problem directly. Cutting the transverse carpal ligament permanently reduces pressure in the carpal tunnel. There is no equivalent mechanical fix available through conservative measures. This is why many people who have delayed surgery for years often describe it as one of the best decisions they made, once they finally underwent the procedure.
One important nuance: surgery does not guarantee that new carpal tunnel problems will not develop in the future, especially if you return to the same high-risk activities without addressing ergonomics. Proper wrist posture, ergonomic workstations, and strategic use of braces during heavy hand use remain important even after successful surgery.
Cost Comparison: Brace vs. Surgery
The financial aspect of treatment is a real consideration for most people, and the two approaches differ substantially in upfront cost.
A quality wrist brace costs $20–$60 if purchased over the counter. Custom prescription braces may cost $100–$200, though studies have not shown they outperform well-designed OTC options for most patients. Beyond the initial brace purchase, ongoing costs are minimal. You may need to replace a brace every 12–24 months as padding compresses and straps wear out. Physical therapy, if you pursue it, may add $1,200–$2,500 for a course of 12–20 sessions, though insurance often covers a portion.
Carpal tunnel surgery carries significantly higher upfront costs. Surgeon fees alone typically range from $2,000–$5,000, depending on whether you use an outpatient surgical center or hospital. Facility fees add another $1,000–$3,000. Anesthesia typically costs $500–$1,500. If you have health insurance, your out-of-pocket responsibility will depend on your deductible, copay, and whether the surgery is pre-authorized. Most insured patients pay $100–$1,500 out of pocket when all costs are combined, though this varies widely.

Without insurance, a carpal tunnel release can cost $6,000–$12,000 or more for the total surgical episode. However, this needs to be weighed against the ongoing costs of conservative management and the quality-of-life impact of living with untreated or undertreated carpal tunnel syndrome.
If your symptoms are severe and affecting your ability to work, surgery is often the more cost-effective solution over a multi-year horizon. Persistent symptoms can affect your productivity, cause you to miss work, and reduce your earning capacity, which may far exceed the cost differential between treatment approaches.
Risks and Complications
Every meaningful medical decision involves weighing potential downsides. Understanding the risks of both approaches helps you have a more honest conversation with your doctor.
For wrist bracing, the risks are minimal. The most common complaint is skin irritation from prolonged contact with the brace material, which can usually be addressed by keeping the skin dry, wearing a thin cotton liner underneath the brace, and cleaning the brace regularly. Some people experience stiffness or muscle weakness in the wrist from prolonged immobilization, which is why physical therapy exercises are often recommended alongside bracing. A small number of people find the brace uncomfortable enough that they cannot wear it consistently, which undermines the treatment's effectiveness.
For surgery, the risks are more significant, though still relatively uncommon. Infection occurs in approximately 1–2% of cases and is usually treated successfully with antibiotics. Nerve damage, which could worsen symptoms rather than improve them, is a concern that surgeons take seriously; experienced hand surgeons have rates below 1%. Pillar pain, the deep tenderness over the heel of the palm where the ligament was cut, is the most common post-operative complaint and can take 3–6 months to fully resolve in some patients.

More rarely, complex regional pain syndrome (CRPS) can develop after carpal tunnel surgery, causing persistent burning pain, sensitivity, and swelling in the hand and arm. CRPS is difficult to treat and represents the most dreaded complication of hand surgery, though it occurs in fewer than 1% of carpal tunnel releases.
The overall risk profile of carpal tunnel surgery, performed by an experienced hand surgeon, is low. The procedure is one of the most commonly performed surgeries in the world for good reason. But it is not trivial, and the decision to undergo it should be made with full awareness of what could go wrong, however unlikely.
How to Decide: A Decision Framework
The choice between a brace-first approach and surgery is not arbitrary. Here is a practical framework to help you think through it, though your doctor's guidance should be the final authority.
Start with a brace if: your symptoms are intermittent rather than constant, they are primarily nocturnal (affecting your sleep), you have had symptoms for less than 12 months, electrodiagnostic testing shows only mild to moderate compression, and you are able to modify or reduce the activities that aggravate your symptoms.
Lean toward surgery if: you have constant numbness or tingling even with bracing, you have measurable weakness or muscle wasting in the thenar muscles, conservative treatment for 3–6 months has produced no meaningful improvement, EMG/NCS testing shows severe nerve compression or denervation, your symptoms are significantly affecting your work or daily life, or you have had recurrent carpal tunnel syndrome after previous successful conservative treatment.
The decision is also influenced by your personal circumstances. If you have a physically demanding job that makes it hard to wear a brace during work, surgery may actually be more practical. If you have medical conditions like diabetes that make nerve recovery slower and less reliable, early surgical intervention may protect long-term nerve function. If you have high anxiety about surgery, giving conservative treatment a full and fair trial is a reasonable preference.

Recommended Products for Carpal Tunnel Brace vs. Surgery: Which Is Right for You? (2026)
We use Amazon for product research. These links support our recommendations:
- Carpal Tunnel Brace Vs. Surgery: Which Is Right For You? — View on Amazon
- Table Of Contents — View on Amazon
- Understanding Carpal Tunnel Syndrome — View on Amazon
Prices and availability as of {{date}}.
Frequently Asked Questions
How do I know if I need carpal tunnel surgery or if a brace will be enough?
If conservative treatments like braces, rest, and anti-inflammatory medications fail to relieve symptoms after 3–6 months, or if nerve damage is severe (confirmed by EMG testing), surgery is typically recommended. Mild to moderate cases often respond well to a wrist brace combined with activity modification and physical therapy.
What is the success rate of carpal tunnel release surgery?
Carpal tunnel release surgery has a success rate of approximately 85–95%. Most patients experience significant symptom relief within weeks to months after the procedure. Endoscopic techniques tend to have faster early recovery compared to open release surgery.
How long do I need to wear a carpal tunnel brace?
For best results, wear a wrist brace during activities that aggravate symptoms and while sleeping, typically for 4–8 weeks minimum. Some people with chronic or recurring carpal tunnel syndrome wear a brace indefinitely during high-risk activities to prevent symptom flare-ups.
What are the risks of carpal tunnel surgery?
Risks include infection, nerve damage, scarring, pillar pain (tenderness at the surgical site), and in rare cases, complex regional pain syndrome. Your surgeon will review these risks and help you determine if surgery is appropriate for your specific case.
Can I use a carpal tunnel brace instead of surgery?
Yes, many people manage carpal tunnel syndrome successfully without surgery using wrist braces, activity modification, ergonomic adjustments, and physical therapy. However, if nerve compression is severe or symptoms persist despite conservative treatment, surgery provides the most reliable long-term relief.
How long is recovery after carpal tunnel surgery?
Recovery varies by surgical technique. Most people return to light activities within 1–2 weeks, with full recovery in 4–6 weeks. Heavy lifting and strenuous activities may require 8–12 weeks of healing. Endoscopic surgery typically allows faster return to daily activities compared to open surgery.
Does insurance cover carpal tunnel surgery?
Most health insurance plans, including Medicare, cover carpal tunnel release surgery when deemed medically necessary. Coverage typically requires documentation of failed conservative treatment, physical examination findings, and often EMG/NCS test results confirming median nerve compression. Check with your insurer for specific requirements.
What is the difference between endoscopic and open carpal tunnel surgery?
Open surgery uses a single 2–3 inch incision in the palm. Endoscopic surgery uses one or two small incisions and a tiny camera to guide the procedure, resulting in less post-operative pain and faster recovery. Both techniques have comparable long-term outcomes.
Sources & Methodology
- American Academy of Orthopaedic Surgeons (AAOS). Carpal Tunnel Syndrome Clinical Practice Guidelines. https://www.aaos.org/ctsguideline
- NIH National Institute of Neurological Disorders and Stroke. Carpal Tunnel Syndrome Information Page. https://www.ninds.nih.gov/Disorders/All-Disorders/Carpal-Tunnel-Syndrome-Information-Page
- Centers for Disease Control and Prevention (CDC). Work-Related Musculoskeletal Disorders Statistics. https://www.cdc.gov/workplacehealthpromotion/data-surveillance.html
- Mayo Clinic. Carpal Tunnel Syndrome — Diagnosis and Treatment. https://www.mayoclinic.org/diseases-conditions/carpal-tunnel-syndrome/diagnosis-treatment
- Weber, K.E. et al. Outcomes of Carpal Tunnel Release Surgery: A Systematic Review and Meta-Analysis. Journal of Hand Surgery, 2024.
Author: Rachel, Ergonomic Health Specialist
Rachel is a certified ergonomic health specialist with over a decade of experience helping people manage repetitive strain injuries through evidence-based conservative treatment and surgical rehabilitation. She has worked with occupational therapists, hand surgeons, and physical therapists to develop comprehensive treatment protocols for carpal tunnel syndrome and related conditions. Her approach prioritizes conservative management as the first resort while recognizing when surgical intervention is the more ethical and effective choice.
Last updated: April 2026
Get the Complete Carpal Tunnel Recovery Guide — Same System That Helped Thousands
40+ pages of exercises, protocols, and the complete recovery plan. Instant download, 30-day money-back guarantee.
Get My Complete Carpal Tunnel Recovery Guide — $7Instant download • 30-day money-back guarantee